Here is the edited text:
A nurse is caring for a client who has a traumatic brain injury. The nurse notes that the client has a widening pulse pressure. Which of the following actions should the nurse take?
Administer a vasodilator medication.
Elevate the head of the bed to 30°.
Apply a cold compress to the forehead.
Decrease the oxygen flow rate.
The Correct Answer is B
Choice A Reason: This choice is incorrect because administering a vasodilator medication may lower the blood pressure and worsen the cerebral perfusion. A vasodilator medication is a drug that relaxes the blood vessels and reduces the resistance to blood flow. It may be used for clients who have hypertension, angina, or heart failure, but it does not help to reduce the intracranial pressure (ICP).
Choice B Reason: This choice is correct because elevating the head of the bed to 30° may help to improve the venous drainage and decrease the ICP. ICP is the pressure exerted by the brain tissue, cerebrospinal fluid (CSF), and blood within the cranial cavity. A normal ICP range is 5 to 15 mm Hg, and an elevated ICP (>20 mm Hg) can cause cerebral ischemia, herniation, or death. Therefore, positioning the client in a semi-Fowler's position (30° angle) or high- Fowler's position (60° to 90° angle) can facilitate breathing and prevent further complications.
Choice C Reason: This choice is incorrect because applying a cold compress to the forehead may cause vasoconstriction and increase the ICP. A cold compress is a device that applies cold temperature to a body part to reduce inflammation, pain, or swelling. It may be used for clients who have headaches, sprains, or bruises, but it does not help to reduce the ICP.
Choice D Reason: This choice is incorrect because decreasing the oxygen flow rate may cause hypoxia and worsen the cerebral ischemia. Hypoxia is a condition in which the body or a part of it does not receive enough oxygen. It may cause symptoms such as confusion, agitation, or cyanosis. Therefore, providing adequate oxygenation and ventilation is essential to maintain the brain function and prevent further damage.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Choice A Reason: This choice is incorrect because urinary hesitancy is not the priority finding for the nurse to address.
Urinary hesitancy is a difficulty or delay in starting or maintaining a urine stream. It may be caused by various factors such as prostate enlargement, urinary tract infection, medication side effects, or psychological issues. It may cause discomfort, pain, or urinary retention, but it does not pose an immediate threat to the client's life.
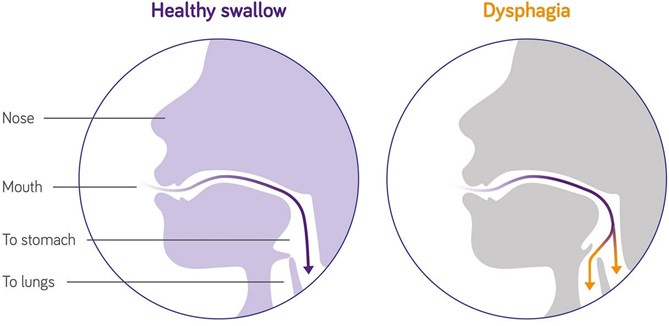
ChoiceB Reason: This choice is correct because dysphagia is the priority finding for the nurse to address. Dysphagia is a difficulty or inability to swallow food or liquids. It may be caused by various factors such as stroke, Parkinson's disease, dementia, esophageal cancer, or oral infections. It may cause malnutrition, dehydration, aspiration, or choking, which can lead to serious complications such as pneumonia, sepsis, or death. Therefore, the nurse should assess the client's swallowing function and provide appropriate interventions such as modifying the diet texture, using thickening agents, or teaching swallowing techniques.
ChoiceC Reason: This choice is incorrect because swollen gums are not the priority finding for the nurse to address. Swollen gums are an inflammation or enlargement of the gingival tissue that surrounds the teeth. They may be caused by various factors such as poor oral hygiene, gum disease, vitamin deficiency, medication side effects, or hormonal changes. They may cause bleeding, pain, or infection, but they do not pose an immediate threat to the client's life.
Choice D Reason: This choice is incorrect because pruritus is not the priority finding for the nurse to address. Pruritus is a sensation of itching that affects the skin. It may be caused by various factors such as dry skin, allergies, eczema, psoriasis, liver disease, or kidney disease. It may cause discomfort, scratching, or skin damage, but it does not pose an immediate threat to the client's life.
Correct Answer is C
Explanation
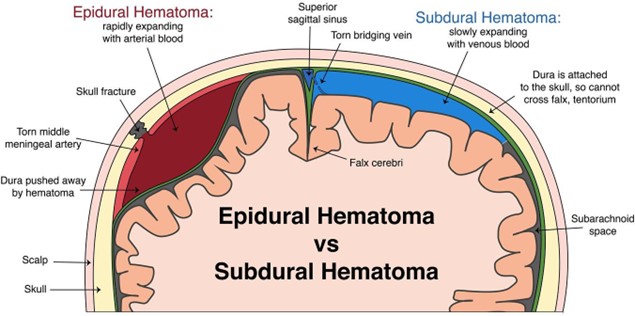
Choice A Reason: Albumin 25% is not a medication that the nurse should plan to administer for a client who is experiencing Cushing's triad following a subdural hematoma. Albumin 25% is a colloid solution that increases the oncotic pressure and draws fluid from the interstitial space into the intravascular space, which can worsen the intracranial pressure by increasing the cerebral blood flow and edema.
Choice B Reason: Dextran 70 is not a medication that the nurse should plan to administer for a client who is experiencing Cushing's triad following a subdural hematoma. Dextran 70 is a plasma expander that increases the blood volume and viscosity, which can also worsen the intracranial pressure by increasing the cerebral blood flow and edema.
Choice C Reason: Mannitol 25% is a medication that the nurse should plan to administer for a client who is experiencing Cushing's triad following a subdural hematoma. Mannitol 25% is an osmotic diuretic that reduces the intracranial pressure by creating an osmotic gradient and drawing fluid from the brain tissue into the blood vessels, which can then be excreted by the kidneys. The nurse should monitor the urine output, serum osmolality, and electrolytes when administering mannitol 25%.
Choice D Reason: Hydroxyethyl starch is not a medication that the nurse should plan to administer for a client who is experiencing Cushing's triad following a subdural hematoma. Hydroxyethyl starch is another plasma expander that has similar effects as dextran 70, and can also increase the risk of coagulopathy and renal failure.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today