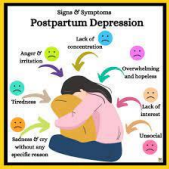
The nurse is assessing a client with postpartum depression for changes in the mood and cognitive state. Which subjective finding(s) should the nurse identify that are consistent with postpartum depression? Select all that apply.
Disrupted sleep.
Grandiosity.
Poor concentration.
Compulsive behavior.
Sadness
Correct Answer : A,C,E
Choice A rationale: Disrupted sleep is a common symptom of postpartum depression, and clients may experience difficulty falling asleep or staying asleep.
Choice B rationale: Grandiosity is more indicative of bipolar disorder (mania) rather than postpartum depression.
Choice C rationale: Poor concentration is a common cognitive symptom associated with postpartum depression.
Choice D rationale: Compulsive behavior is not typically associated with postpartum depression.
Choice E rationale: Sadness is a hallmark symptom of depression, including postpartum depression.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
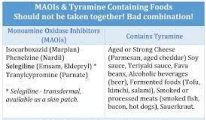
Choice A rationale: Hydrochlorothiazide is a diuretic and may contribute to electrolyte imbalances, but it is not the most concerning medication in this situation. Choice B rationale: Phenelzine is a monoamine oxidase inhibitor (MAOI), and the combination of an MAOI with certain foods or medications containing tyramine can lead
to a hypertensive crisis. The client's elevated blood pressure is of concern, and the nurse should notify the healthcare provider.
Choice C rationale: Losartan is an angiotensin II receptor blocker (ARB) used to treat hypertension. While it may contribute to blood pressure control, it is not the most concerning medication in this scenario.
Choice D rationale: Aspirin, at a dose of 81 milligrams, is often used for cardiovascular prophylaxis and is not the most concerning medication in this situation.
Correct Answer is D
Explanation
Choice A rationale: Asking in a non-threatening manner why the client cut their own abdomen is an appropriate therapeutic communication technique but may not be the priority during a dressing change. Safety and hygiene are essential.
Choice B rationale: Providing detailed thorough explanations when cleansing the wound is valuable, but the nurse should prioritize the physical care and safety aspects of the dressing change.
Choice C rationale: Requesting another staff member to assist with the dressing change may be appropriate for some clients, but it may not be necessary for every situation. The nurse should be capable of performing the dressing change safely. Choice D rationale: Performing the dressing change in a non-judgmental manner is crucial. The nurse should focus on providing care in a sensitive and non-critical way to establish trust and ensure the client's physical well-being.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today