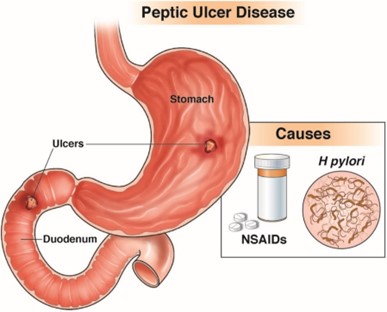
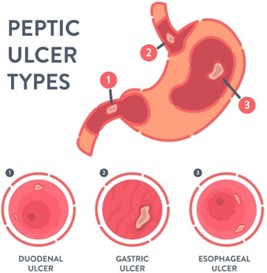
The nurse is caring for a client with diagnosis of peptic ulcer disease. Which assessment finding indicates to the nurse that the client most likely has an ulcer in the stomach rather than the duodenum?
The client's stool is positive for occult blood.
The client reports abdominal discomfort an hour after each meal.
The client has had four ulcers in the last 5 years.
The client's hemoglobin is 13 g/dL and hematocrit is 42%.
The Correct Answer is B
Abdominal discomfort an hour after a meal is a common symptom of a gastric ulcer because the stomach is where food is initially processed, and stomach acid is most concentrated. In contrast, duodenal ulcers typically cause pain 2-3 hours after meals, as food moves out of the stomach and into the duodenum, where it encounters duodenal acid.
A positive stool occult blood test is a non-specific finding that can be caused by many gastrointestinal conditions, including peptic ulcers. It does not indicate the location of the ulcer.
The number of ulcers the client has had in the past does not indicate the location of the current ulcer.
Normal hemoglobin and hematocrit levels do not provide information about the location of the ulcer.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
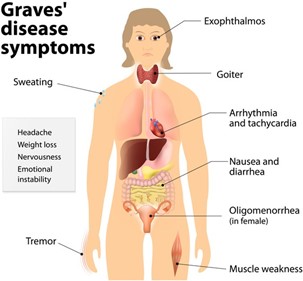
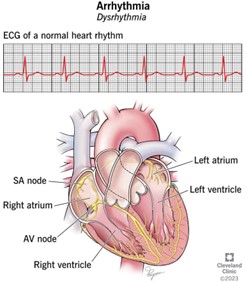
The patient's bounding, rapid pulse and systolic hypertension may indicate cardiovascular complications associated with Graves' disease, such as tachycardia, atrial fibrillation, or congestive heart failure, which can cause chest pain. It is important for the nurse to assess for any symptoms of cardiovascular distress and report any abnormal findings to the healthcare provider for prompt intervention. Questions about appetite and constipation may be relevant to the patient's overall health status, but they are not the most important concern in this situation.
Correct Answer is A
Explanation
The plan of care for a patient with hypothermia and fluid volume excess would typically include measures to increase the patient's body temperature and decrease their fluid volume. Therefore, option a (fluid restriction) would be appropriate for this patient.
Options b (administration of hypotonic IV fluids) and d (administration of ion-exchange resin) would not be appropriate because they would increase the patient's fluid volume rather than decrease it.
Option c (placement of an indwelling urinary catheter) may be appropriate to closely monitor the patient's urine output, which is an important indicator of their fluid status. However, this alone would not be sufficient to manage the patient's hypothermia and fluid volume excess.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today