While assessing the newborn, the nurse should be aware that the average expected apical pulse range of a full-term, quiet, alert newborn is __ beats/min.
100 to 120
120 to 160
80 to 100
150 to 180
The Correct Answer is B
Choice a) 100 to 120 is incorrect because this is too low for a normal newborn's heart rate. The heart rate of a newborn is influenced by factors such as gestational age, activity level, temperature, and health status. A full-term, quiet, alert newborn should have a heart rate between 120 and 160 beats per minute, which reflects their high metabolic rate and oxygen demand. A heart rate below 100 beats per minute may indicate bradycardia, which can be caused by hypoxia, hypothermia, or cardiac problems.
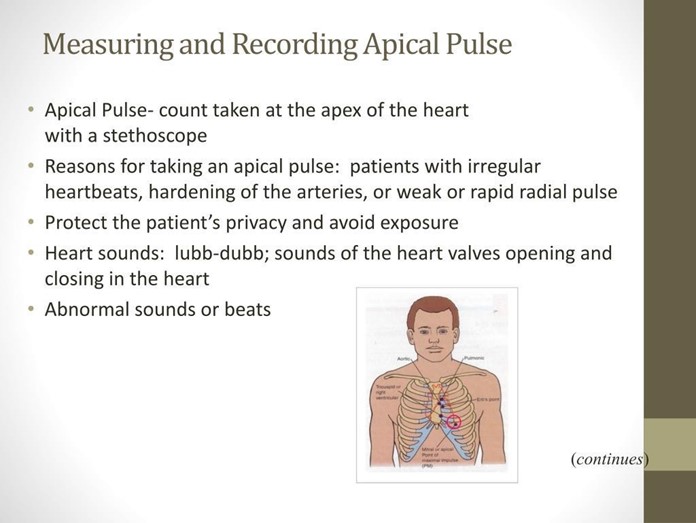
Choice b) 120 to 160 is correct because this is the normal range for a full-term, quiet, alert newborn's heart rate. The apical pulse is the best way to measure the heart rate of a newborn, as it reflects the actual contractions of the heart. The apical pulse can be auscultated at the fourth intercostal space on the left side of the chest, just below the nipple line. The nurse should count the apical pulse for a full minute, as it may vary with the respiratory cycle.
Choice c) 80 to 100 is incorrect because this is also too low for a normal newborn's heart rate. A full-term, quiet, alert newborn should have a heart rate between 120 and 160 beats per minute, which is higher than that of an adult or an older child. A heart rate below 100 beats per minute may indicate bradycardia, which can be caused by hypoxia, hypothermia, or cardiac problems.
Choice d) 150 to 180 is incorrect because this is too high for a normal newborn's heart rate. A full-term, quiet, alert newborn should have a heart rate between 120 and 160 beats per minute, which is lower than that of a preterm or a crying newborn. A heart rate above 160 beats per minute may indicate tachycardia, which can be caused by fever, infection, anemia, or hyperthyroidism.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
Choice a) We are protecting the infant from our bacteria is incorrect because this is not the main reason why gloves are needed when handling a newborn. While it is true that newborns have immature immune systems and are susceptible to infections, gloves are not only used to protect the infant from our bacteria but also to protect ourselves from the infant's body fluids and secretions, which may contain pathogens or blood-borne diseases.
Therefore, this response is incomplete and misleading.
Choice b) Amniotic fluid and maternal blood pose risks to us is incorrect because this is also not the primary reason why gloves are needed when handling a newborn. While it is true that amniotic fluid and maternal blood may contain harmful microorganisms or viruses that can infect us, gloves are not only used to protect ourselves from these substances but also to protect the infant from our skin flora and potential contaminants, which may cause skin irritation or infection. Therefore, this response is also incomplete and misleading.
Choice c) It is hospital policy is incorrect because this is not a sufficient or satisfactory reason why gloves are needed when handling a newborn. While it is true that wearing gloves may be a hospital policy or protocol, this response does not explain the rationale or evidence behind this policy and may imply that the nurse does not understand or agree with it. Therefore, this response is vague and unprofessional.
Choice d) It is part of standard precautions is correct because this is the best and most accurate reason why gloves are needed when handling a newborn. Standard precautions are a set of guidelines and practices that aim to prevent the transmission of infections in healthcare settings. They include wearing gloves, gowns, masks, and eye protection when there is a risk of exposure to blood or body fluids, as well as washing hands before and after patient contact, cleaning and disinfecting equipment and surfaces, and disposing of waste properly. Standard precautions apply to all patients, regardless of their diagnosis or infection status, and are based on the principle that all blood and body fluids are potentially infectious. Therefore, this response is clear and appropriate.
Correct Answer is C
Explanation
Choice a) Breasts firm and tender is incorrect because this is not a sign of normal involution, but rather a sign of breast engorgement, which is a common problem in the first few weeks of breastfeeding. Breast engorgement occurs when thE breasts become overfilled with milk, causing them to feel hard, swollen, painful, and warm. It can be prevented or relieved by frequent and effective breastfeeding, applying warm or cold compresses, massaging the breasts, expressing some milk, and wearing a supportive bra.
Choice b) Episiotomy slightly red and puffy is incorrect because this is not a sign of normal involution, but rather a sign of inflammation or infection of the perineal wound. An episiotomy is a surgical cut made in the perineum (the area between the vagina and the anus) to enlarge the vaginal opening during delivery. It can take several weeks to heal and may cause pain, swelling, bruising, bleeding, or discharge. It can be cared for by keeping the area clean and dry, applying ice packs or witch hazel pads, taking painkillers or sitz baths, and avoiding constipation or straining.
Choice c) Fundus below the symphysis and not palpable is correct because this is a sign of normal involution, which is the process of the uterus returning to its pre-pregnancy size and shape after delivery. The fundus is the upper part of the uterus that can be felt through the abdomen. Immediately after delivery, the fundus is about the size of a grapefruit and can be felt at or above the umbilicus (the navel). It gradually descends about one fingerbreadth per day until it reaches the level of the symphysis pubis (the joint where the two pubic bones meet) by about 10 days postpartum. By 14 days postpartum, the fundus should be below the symphysis and not palpable.
Choice d) Moderate bright red lochial flow is incorrect because this is not a sign of normal involution, but rather a sign of excessive or prolonged bleeding after delivery. Lochia is the vaginal discharge that consists of blood, mucus, and tissue from the lining of the uterus. It changes in color and amount over time, from red to pink to brown to yellow to white. The normal lochia flow should be scant to moderate in amount, dark red to brown in color, and last for about 4 to 6 weeks postpartum. A moderate bright red lochial flow on day 14 postpartum may indicate that the uterus is not contracting well or that there is an infection or retained placental tissue in the uterus.

Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today