A nurse at a community health clinic is planning care for an adolescent who recently learned that she is pregnant and is concerned about her ability to afford and care for her baby. Which of the following actions should the nurse take?
Contact the adolescent’s parent for assistance.
Assist the adolescent in applying for Medicaid.
Refer the adolescent to a local mental health clinic.
Advise the adolescent to place the newborn for adoption.
The Correct Answer is B
The correct answer is B.
Assist the adolescent in applying for Medicaid.
This action demonstrates the nurse’s role as an advocate and a resource person for the client, who might be eligible for financial assistance and health care coverage during her pregnancy and postpartum period. Medicaid is a federal and state program that provides health insurance for low-income individuals and families.
Choice A is wrong because contacting the adolescent’s parent for assistance might violate the client’s confidentiality and autonomy, especially if the parent is not aware of or supportive of the pregnancy. The nurse should respect the client’s right to privacy and self-determination, unless there is a risk of harm to the client or the fetus.
Choice C is wrong because referring the adolescent to a local mental health clinic might imply that the client has a mental disorder or needs psychological counseling, which could be stigmatizing and discouraging.
The nurse should assess the client’s emotional state and coping skills, and provide supportive and nonjudgmental care. The nurse can also offer referrals to other community resources, such as prenatal education, parenting classes, or social services, that might benefit the client.
Choice D is wrong because advising the adolescent to place the newborn for adoption might interfere with the client’s decision-making process and personal values.
The nurse should not impose his or her own opinions or beliefs on the client, but rather explore the client’s feelings and preferences about her pregnancy options. The nurse should provide factual information and education about adoption, abortion, or parenting, and help the client weigh the benefits and risks of each option.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
This is a sign of preeclampsia, a serious complication of pregnancy that can cause high blood pressure, proteinuria, and seizures.
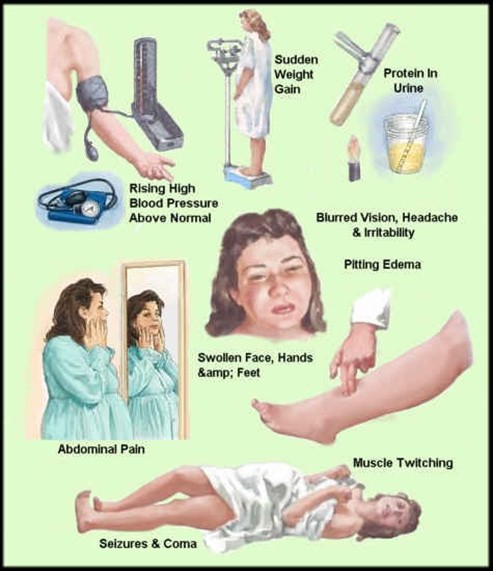
Preeclampsia can affect the placenta, the kidneys, the liver, and the brain of the mother and the fetus. It requires immediate medical attention and may lead to early delivery.
Choice A, bleeding gums, is wrong because it is a common occurrence during pregnancy due to hormonal changes that increase blood flow to the gums. It is not a cause for concern unless it is excessive or accompanied by other symptoms.
Choice B, urinary frequency, is wrong because it is also a normal finding during pregnancy due to the growing uterus putting pressure on the bladder. It is not a sign of infection or kidney problems unless it is associated with pain, burning, or blood in the urine.
Choice D, faintness upon rising, is wrong because it is usually caused by orthostatic hypotension, a drop in blood pressure when changing positions.
This can happen during pregnancy due to the dilation of blood vessels and the increased blood volume. It can be prevented by rising slowly, drinking enough fluids, and avoiding prolonged standing.
Correct Answer is B
Explanation
The correct answer is choice B. Increase exercise.
Exercise can help stimulate bowel movements and prevent constipation, which is a common side effect of opioid medications.
Exercise can also improve blood circulation, reduce stress, and enhance mood, which can benefit clients who have chronic pain.
Choice A is wrong because decreasing insoluble fiber intake can worsen constipation.
Insoluble fiber adds bulk to the stool and helps it pass more easily through the colon.
Clients who take opioid medications should increase their intake of insoluble fiber from sources such as whole grains, fruits, vegetables, nuts, and seeds.
Choice C is wrong because drinking less water can lead to dehydration and hardening of the stool, which can make it more difficult to pass.
Clients who take opioid medications should drink plenty of water to keep the stool soft and moist.
Choice D is wrong because taking a laxative every day can cause dependence, tolerance, and electrolyte imbalance.
Laxatives should be used only as a last resort and under the guidance of a health care provider.
Clients who take opioid medications should try other methods of preventing constipation first, such as increasing exercise, fiber, and water intake.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today