The nurse will conduct what assessment on a newborn at 1 minute and 5 minutes after birth?
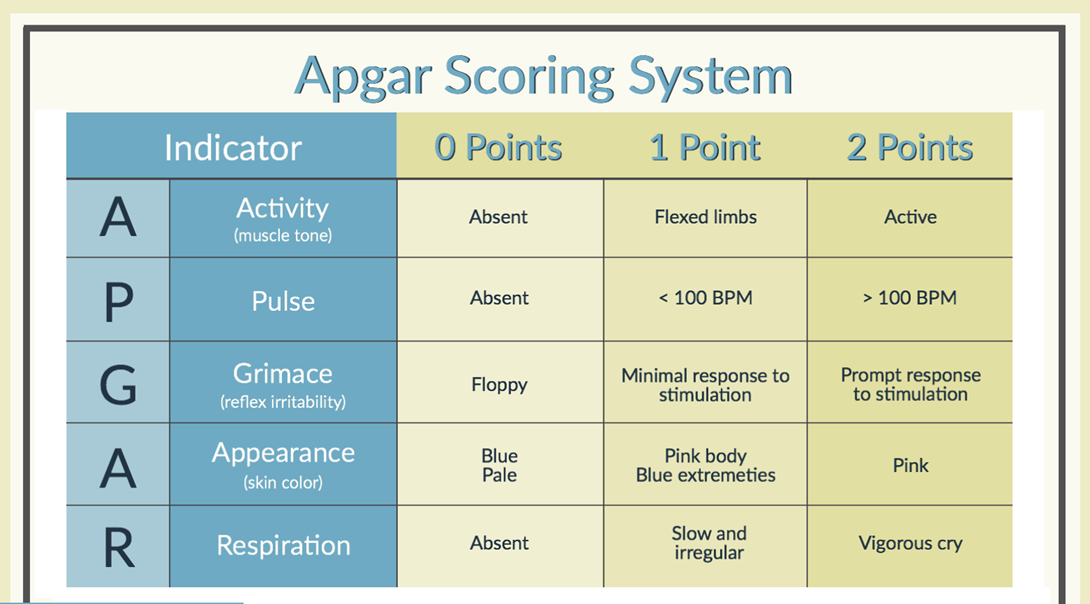
Apgar score
Blood pressure reading
Head and chest circumference
Respiratory and abdominal assessment
The Correct Answer is A
Choice A reason: This is the best answer. Apgar score is a quick and simple assessment that evaluates the newborn's appearance, pulse, grimace, activity, and respiration. It is done at 1 minute and 5 minutes after birth, and sometimes at 10 minutes if needed. It helps to determine the newborn's condition and need for resuscitation or medical intervention.
Choice B reason: This is not the correct answer. Blood pressure reading is a measurement of the force of the blood against the walls of the arteries. It is not routinely done on newborns, unless there is a suspicion of a cardiac or renal problem. It is usually done after the first 24 hours of life, and then as indicated by the newborn's condition.
Choice C reason: This is not the correct answer. Head and chest circumference are measurements of the size and shape of the newborn's head and chest. They are done once within the first 24 hours of life, and then as indicated by the newborn's condition. They help to monitor the newborn's growth and development, and to detect any abnormalities or asymmetries.
Choice D reason: This is not the correct answer. Respiratory and abdominal assessment are examinations of the newborn's breathing and digestion. They are done once within the first 24 hours of life, and then as indicated by the newborn's condition. They help to evaluate the newborn's lung and bowel function, and to identify any signs of distress or complications.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
Choice A reason: This is not the statement that the nurse will prioritize. The client may want the instructions written out for convenience or clarity, but it does not indicate their level of self-efficacy.
Choice B reason: This is not the statement that the nurse will prioritize. The client may not have changed the dressing by themselves yet, but it does not mean that they cannot do it. The client may just need more practice or guidance.
Choice C reason: This is not the statement that the nurse will prioritize. The client may want their son to help them for emotional or physical support, but it does not reflect their self-efficacy.
Choice D reason: This is the statement that the nurse will prioritize. The client expresses a negative belief about their ability to perform the dressing change. This indicates that the client has low self-efficacy, which is the confidence in one's ability to accomplish a specific task. The nurse should address this statement by providing positive feedback, encouragement, and reassurance to the client. The nurse should also demonstrate the steps of the dressing change and allow the client to practice under supervision.
Correct Answer is D
Explanation
Choice A reason: This is not an indicator of appropriate neurological development. Appropriate weight is a measure of the physical growth and nutritional status of the baby. It is influenced by the baby's genetics, gestational age, birth weight, feeding habits, and health conditions. Appropriate weight does not reflect the baby's brain development or function.
Choice B reason: This is not an indicator of appropriate neurological development. Vernix caseosa is a white, cheesy substance that covers the skin of the baby in the womb. It protects the skin from the amniotic fluid and helps with temperature regulation and infection prevention. Vernix caseosa is mostly shed before or during birth, and does not relate to the baby's brain development or function.
Choice C reason: This is not an indicator of appropriate neurological development. Presence of lanugo is a fine, soft hair that covers the body of the baby in the womb. It helps to keep the baby warm and hold the vernix caseosa on the skin. Presence of lanugo is usually lost before or shortly after birth, and does not indicate the baby's brain development or function.
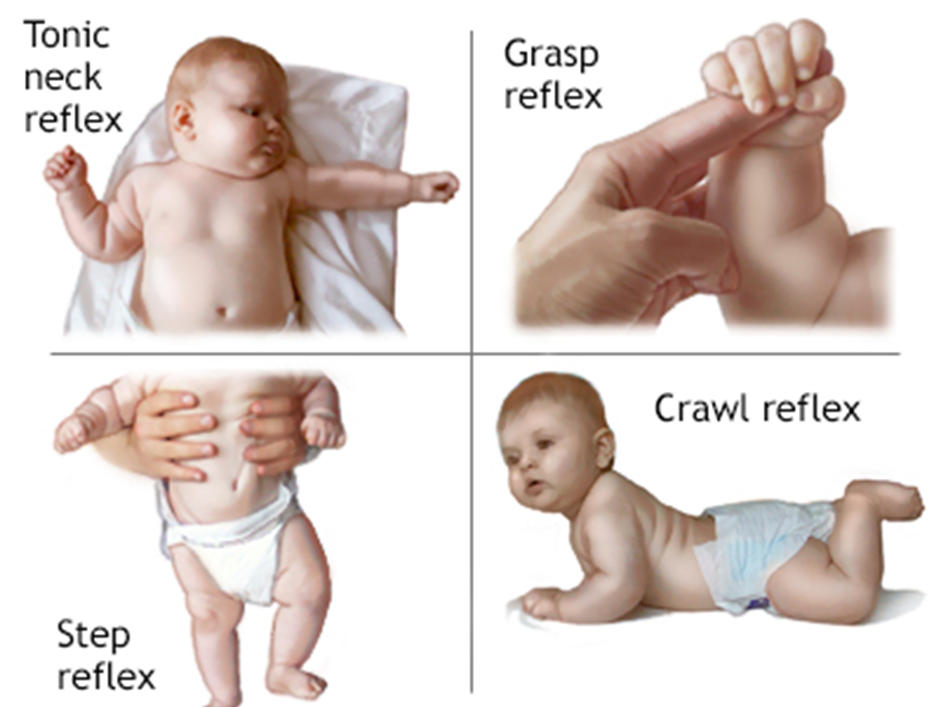
Choice D reason: This is the best answer. Expected reflexes are involuntary movements or responses that the baby makes in reaction to certain stimuli. They are controlled by the nervous system and indicate the baby's brain development and function. Expected reflexes include the rooting, sucking, grasping, Moro, and Babinski reflexes. The nurse should assess the presence, strength, and symmetry of these reflexes during the well-baby check.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today