The nurse is discussing the steps of a dressing change with a client who has low self-efficacy. What statement by the client will the nurse prioritize?
"I want the instructions written out."
"I haven't changed the dressing by myself yet."
"I want my son to help me."
"I don't think I can do this."
The Correct Answer is D
Choice A reason: This is not the statement that the nurse will prioritize. The client may want the instructions written out for convenience or clarity, but it does not indicate their level of self-efficacy.
Choice B reason: This is not the statement that the nurse will prioritize. The client may not have changed the dressing by themselves yet, but it does not mean that they cannot do it. The client may just need more practice or guidance.
Choice C reason: This is not the statement that the nurse will prioritize. The client may want their son to help them for emotional or physical support, but it does not reflect their self-efficacy.
Choice D reason: This is the statement that the nurse will prioritize. The client expresses a negative belief about their ability to perform the dressing change. This indicates that the client has low self-efficacy, which is the confidence in one's ability to accomplish a specific task. The nurse should address this statement by providing positive feedback, encouragement, and reassurance to the client. The nurse should also demonstrate the steps of the dressing change and allow the client to practice under supervision.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
Choice A reason: This is not the client who has an increased risk for body-image disturbance. A cardiac catheterization is a procedure that involves inserting a thin tube into a blood vessel and guiding it to the heart. It is used to diagnose or treat heart problems. It does not cause any visible changes to the body or affect the client's appearance or function.
Choice B reason: This is not the client who has an increased risk for body-image disturbance. An appendectomy is a surgery that involves removing the appendix, which is a small pouch attached to the large intestine. It is used to treat appendicitis, which is an inflammation of the appendix. It does not cause any significant changes to the body or affect the client's appearance or function.
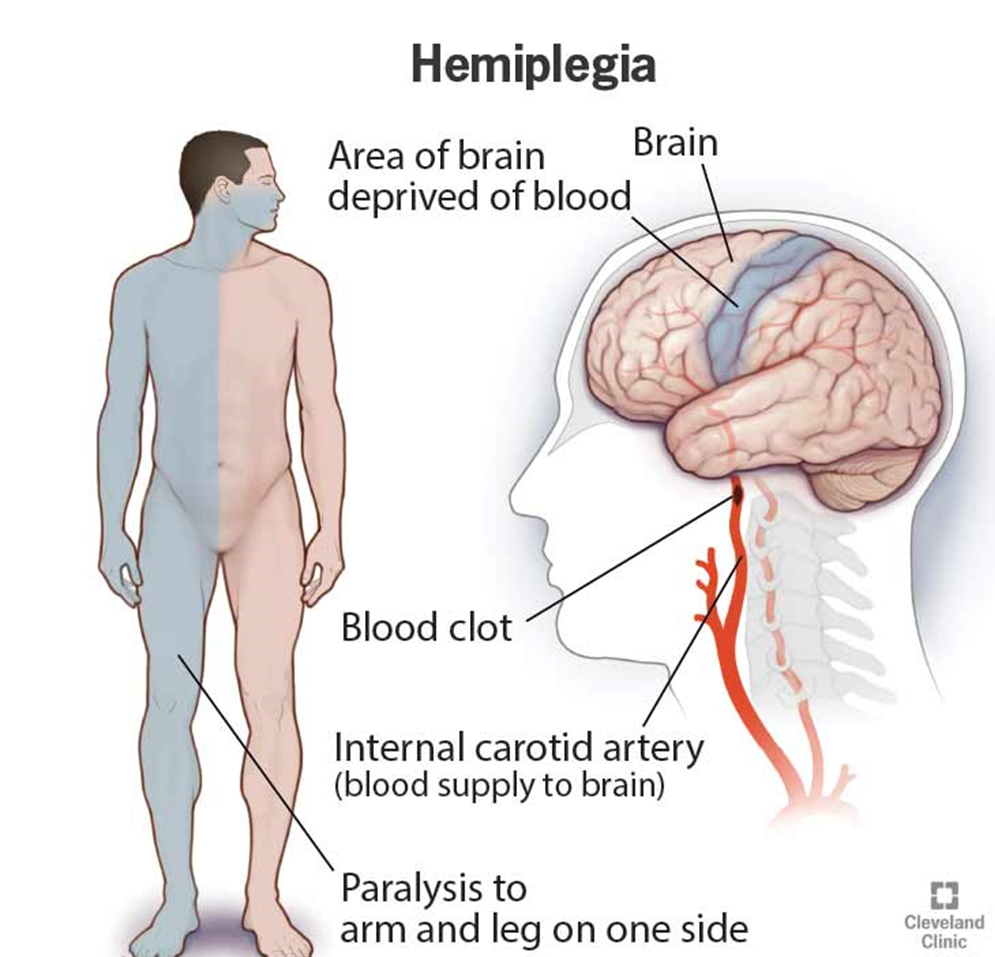
Choice C reason: This is the client who has an increased risk for body-image disturbance. A stroke is a condition that occurs when the blood supply to a part of the brain is interrupted, causing brain cells to die. It can cause various neurological impairments, depending on the location and severity of the damage. Left-sided hemiplegia is a paralysis of the left side of the body, which can affect the client's movement, sensation, speech, and facial expression. It can cause a noticeable change to the body and affect the client's appearance and function.
Choice D reason: This is not the client who has an increased risk for body-image disturbance. Shoulder surgery is a surgery that involves repairing or replacing the structures of the shoulder joint, such as the bones, muscles, tendons, or ligaments. It is used to treat shoulder injuries or disorders, such as fractures, dislocations, arthritis, or rotator cuff tears. It does not cause any major changes to the body or affect the client's appearance or function.
Correct Answer is D
Explanation
Choice A reason: This is not the correct answer. Autonomy vs. Shame and Doubt is the psychosocial developmental stage that occurs in toddlers, who are between 1 and 3 years old. It involves the development of independence and self-control, as well as the awareness of personal limitations and expectations. The nurse should encourage parents of toddlers to provide them with choices, boundaries, and praise, and to avoid overprotection, criticism, or ridicule.
Choice B reason: This is not the correct answer. Initiative vs. Guilt is the psychosocial developmental stage that occurs in preschoolers, who are between 3 and 5 years old. It involves the development of initiative and creativity, as well as the sense of responsibility and morality. The nurse should encourage parents of preschoolers to provide them with opportunities, guidance, and feedback, and to avoid discouragement, punishment, or interference.
Choice C reason: This is not the correct answer. Intimacy vs. Isolation is the psychosocial developmental stage that occurs in young adults, who are between 18 and 39 years old. It involves the development of intimacy and commitment, as well as the ability to form and maintain close relationships. The nurse should encourage young adults to explore their identity, values, and goals, and to seek and offer support, trust, and love.
Choice D reason: This is the best answer. Trust vs. Mistrust is the psychosocial developmental stage that occurs in infants, who are between birth and 1 year old. It involves the development of trust and security, as well as the attachment and bonding with the caregivers. The nurse should encourage parents of infants to feed the baby when hungry and comfort the baby when crying, as well as to provide them with consistent, responsive, and loving care.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today