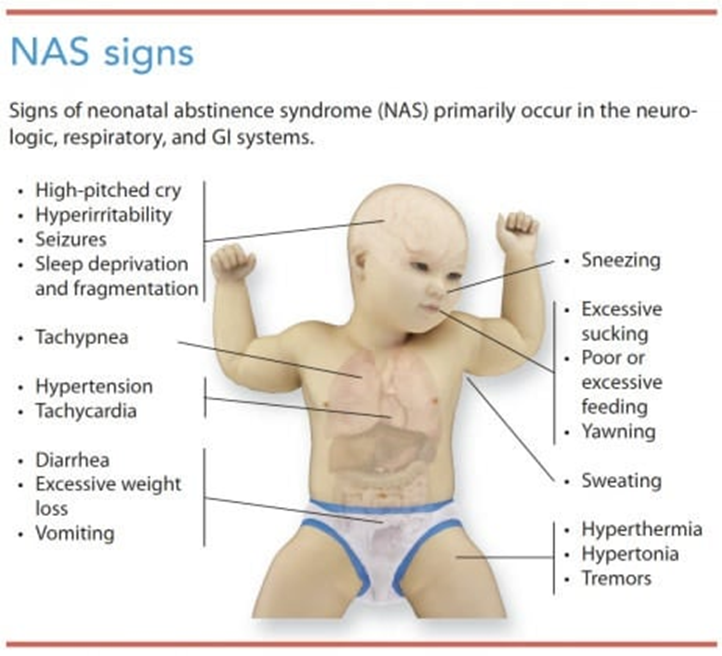
A neonate born to a mother who was abusing heroin is exhibiting signs and symptoms of withdrawal. Which signs would the nurse assess? (Select All that Apply.)
hypertonicity
excessive sneezing
low whimpering cry
overly vigorous sucking
lethargy
tremors
Correct Answer : A,B,C,D,E,F
A. Hypertonicity: Neonates experiencing withdrawal from heroin may exhibit increased muscle tone, leading to stiffness or rigidity. This is often observed as hypertonicity in their limbs or overall body.
B. Excessive sneezing: Nasal congestion and sneezing are common symptoms in neonates undergoing withdrawal. These symptoms can occur due to the irritant effects of withdrawal on the respiratory system.
C. Low whimpering cry: Infants with neonatal abstinence syndrome (NAS) may have a weak or high-pitched cry, which may sound like whimpering. This cry can be indicative of the discomfort and distress they are experiencing.
D. Overly vigorous sucking: Neonates with NAS may display exaggerated sucking behaviors, often characterized by frantic or overly vigorous sucking during feeding or when provided with a pacifier. This behavior is a manifestation of their heightened agitation and irritability.
E. Lethargy: Some neonates experiencing NAS may appear excessively drowsy, fatigued, or have decreased responsiveness. Lethargy is a common symptom associated with withdrawal from heroin or other opioids.
F. Tremors: Tremors or shaking movements, especially when the neonate is disturbed or agitated, are hallmark signs of NAS. These tremors can be mild to severe and may affect various parts of the body, such as the arms, legs, or jaw.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
A. Oligohydramnios:
Oligohydramnios refers to a condition where there is too little amniotic fluid surrounding the fetus in the womb. It can be concerning because amniotic fluid plays a crucial role in protecting and cushioning the fetus, aiding in lung development, and preventing compression of the umbilical cord. While oligohydramnios can be a complication in pregnancy, it's not necessarily more common or specific to twin pregnancies compared to singleton pregnancies.
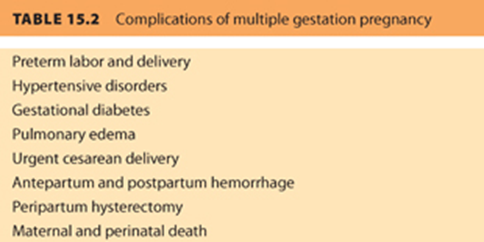
B. Preeclampsia:
Preeclampsia is a serious pregnancy complication characterized by high blood pressure and signs of damage to other organ systems, such as the liver and kidneys. It usually develops after 20 weeks of pregnancy and can lead to serious complications for both the mother and the babies if not managed properly. Multiple pregnancies, including twins, are considered a risk factor for developing preeclampsia. Therefore, pregnant women carrying twins require close monitoring for signs and symptoms of preeclampsia.
C. Chorioamnionitis:
Chorioamnionitis is an infection of the fetal membranes (chorion and amnion) and amniotic fluid. It typically occurs due to bacterial infection ascending from the vagina into the uterus, often during prolonged labor or rupture of membranes. While chorioamnionitis is a concern in pregnancy, it's not necessarily more common in twin pregnancies compared to singleton pregnancies.
D. Post-term labor:
Post-term labor refers to labor that begins after 42 weeks of gestation. Prolonged pregnancy beyond the due date can increase the risks of complications for both the mother and the baby, including fetal distress, macrosomia (large birth weight), and meconium aspiration. Post-term labor can occur in both singleton and multiple pregnancies, but it's not specifically more associated with twin pregnancies.
Correct Answer is C
Explanation
A. Attach a sign above her bed to have BP, IV lines, and lab work in her right arm.
- This option is not appropriate because after a right-sided modified-radical mastectomy, it's generally contraindicated to use the affected arm (right arm in this case) for blood pressure measurements, IV lines, or blood draws. This is because such procedures can impede lymphatic drainage and increase the risk of lymphedema. Therefore, the unaffected arm is typically preferred for these purposes to reduce the risk of complications.
B. Encourage her to turn, cough, and deep breathe at frequent intervals.
- While turning, coughing, and deep breathing are essential postoperative nursing interventions to prevent respiratory complications such as pneumonia, they are not specific to the unique needs of a woman who has undergone a mastectomy. These interventions are more focused on general postoperative care rather than addressing the specific concerns related to mastectomy, such as lymphedema management.
C. Position her right arm below heart level.
- This is the correct choice. Positioning the right arm below heart level helps reduce swelling and promotes lymphatic drainage, particularly after surgery involving the lymph nodes, as in a mastectomy. This positioning aids in preventing complications such as lymphedema and supports optimal circulation and fluid balance in the affected arm.
D. Ask the client how she feels about having her breast removed.
- While emotional support and addressing the client's feelings are important aspects of care for a woman who has undergone a mastectomy, this intervention is more appropriate during psychosocial assessment and counseling sessions, rather than immediately postoperatively. At this stage, the focus should be primarily on physical recovery and addressing immediate postoperative needs, such as pain management and prevention of complications like lymphedema. Emotional support can certainly be provided, but it should not be the primary intervention immediately following surgery.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today