
Obsessive-Compulsive and Related Disorders
Lessons
- Objectives
- Introduction
- Overview Of Oc And Related Disorders (Ocrds)
- Obsessions
- Compulsions
- Practice Exercise 1
- Compulsive Behavior Patterns
- Related Disorders
- Practice Exercise 2
- Assessment In Nursing Practice
- Nursing Diagnoses And Planning
- Interventions And Treatments
- Practice Exercise 3
- Complications, Prognosis, And Patient Education
- Summary
- Comprehensive Questions
Notes Highlighting is available once you sign in. Login Here.
Objectives
- Define Obsessive-Compulsive Disorder (OCD) and its core components, including obsessions, compulsions, and related behavioral patterns, based on established diagnostic frameworks.
- Identify epidemiological trends, etiological factors, and neurobiological underpinnings of OCD and associated disorders.
- Differentiate OCD from related disorders like body dysmorphic disorder, hoarding disorder, trichotillomania, and excoriation disorder, focusing on clinical features.
- Apply nursing assessment techniques, including screening tools and cultural considerations, to evaluate patients with these conditions.
- Formulate appropriate nursing diagnoses, plan interventions, and evaluate outcomes using evidence-based treatments like pharmacotherapy and cognitive-behavioral therapy.
- Recognize complications, prognostic indicators, and patient education strategies to promote holistic care and recovery.
- Integrate key nursing insights to enhance clinical decision-making and prepare for nursing examinations on mental health topics.
Introduction
- Obsessive-compulsive and related disorders involve persistent, intrusive thoughts and repetitive behaviors significantly impairing daily functioning.
- These disorders are classified together due to shared features of repetitive, unwanted mental or behavioral activities aimed at reducing distress.
- OCD affects millions globally and often co-occurs with anxiety, depression, or other psychiatric conditions.
- Nurses play a critical role in early identification, therapeutic alliance building, medication management, and supporting behavioral therapies.
Overview Of Oc And Related Disorders (Ocrds)
- OCD is a chronic psychiatric condition characterized by recurrent obsessions and compulsions causing marked distress and functional impairment.
- Related disorders share phenomenological similarities but differ in focus, such as appearance in body dysmorphic disorder or hair-pulling in trichotillomania.
- Dysregulation in cortico-striato-thalamo-cortical circuits, with genetic, environmental, and neurochemical influences, underpins these disorders.
- Prevalence of OCD is approximately 1-3% globally, highlighting the need for nursing proficiency in recognition and management.
1.1 Definition and Diagnostic Features
- OCD is defined by the presence of obsessions, compulsions, or both, which are time-consuming (more than one hour per day) and not attributable to another medical condition or substance use.
- Diagnostic features include recognition by the individual that obsessions or compulsions are excessive, though insight may vary.
- Related disorders involve repetitive behaviors directed toward specific foci, such as perceived defects in body dysmorphic disorder.
- Obsessions are recurrent, persistent thoughts, urges, or images that are intrusive and unwanted, causing anxiety or distress.
- Compulsions are repetitive behaviors or mental acts performed in response to obsessions or rigid rules.
- Disorders must cause clinically significant distress or impairment, not better explained by other mental disorders like schizophrenia.
Nursing Insights
- Nurses must recognize that poor insight in OCD (belief that obsessions are realistic) occurs in 25-30% of cases, associated with worse prognosis, guiding tailored interventions and predicting treatment adherence.
1.2 Epidemiology
- OCD has a lifetime prevalence of 2-3%, with onset typically in late adolescence or early adulthood, though childhood onset occurs.
- Females are slightly more affected than males in adulthood; males predominate in pediatric cases.
- Related disorders’ prevalence: body dysmorphic disorder (1-2%), hoarding disorder (2-6%), trichotillomania (1-2%), excoriation disorder (1-5%).
- Cultural factors influence presentation; religious obsessions are common in devout populations.
- Comorbidity is high, with 75% of OCD patients having at least one additional axis I disorder, such as depression or anxiety.
- Risk is elevated in first-degree relatives, with heritability estimates of 40-50% for OCD.
- Socioeconomic factors, urban living, and stressful life events correlate with higher incidence.
- Global studies show consistent core symptoms but variations in content based on cultural norms.
1.3 Etiology and Risk Factors
- Etiology involves genetic, neurobiological, environmental, and psychological factors.
- Genetic factors include candidate genes like serotonin transporter (SLC6A4) and glutamate systems (SLC1A1).
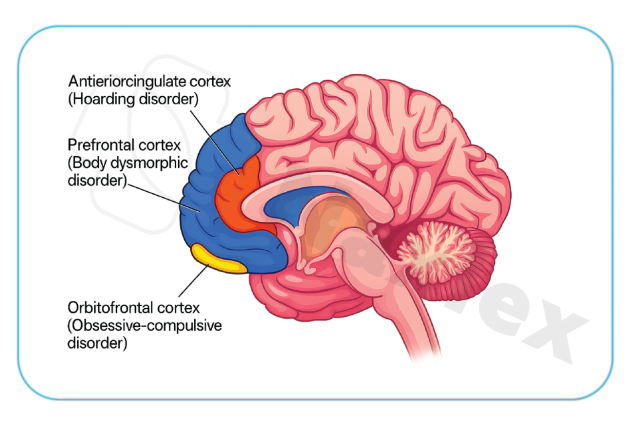
- Neurobiologically, hyperactivity in orbitofrontal cortex, anterior cingulate cortex, and basal ganglia is implicated, shown by functional MRI.
- Environmental risks include perinatal complications, streptococcal infections (PANDAS), and trauma.
- Psychological models, like cognitive appraisal theory, suggest misinterpretation of intrusive thoughts contributes to symptom maintenance.
- Twin studies show 80-87% concordance in monozygotic twins versus 47-50% in dizygotic, supporting heritability.
- Serotonin dysregulation is central, evidenced by SSRI efficacy; dopamine and glutamate also play roles.
- Childhood abuse increases risk by 2-3 times; infections like group A streptococcus can precipitate acute onset in children.
- Protective factors include strong social support and cognitive resilience.
Obsessions
- Obsessions are involuntary mental intrusions provoking anxiety and compelling behavioral responses.
- They arise from dysfunctional beliefs where neutral thoughts are appraised as threatening, leading to amygdala activation and distress.
- Obsessions must be time-consuming and not pleasurable, distinguishing them from ruminations in other disorders.
1.1 Characteristics
- Obsessions are recurrent, persistent thoughts, impulses, or images intruding into consciousness, causing marked anxiety or distress.
- Characteristics include intrusiveness, resistance to suppression, and association with specific themes.
- Individuals attempt to ignore or neutralize obsessions with compulsions, providing temporary relief.
- Persistence: Obsessions recur despite efforts to dismiss, escalating under stress.
- Distress induction: Trigger physiological responses like increased heart rate and cortisol levels.
- Insight variability: Most recognize obsessions as irrational, but poor insight leads to acting as if true.
- Obsessions differ from worries in generalized anxiety disorder by being more image-based and less reality-oriented, vital for differential diagnosis.
1.2 Common Themes
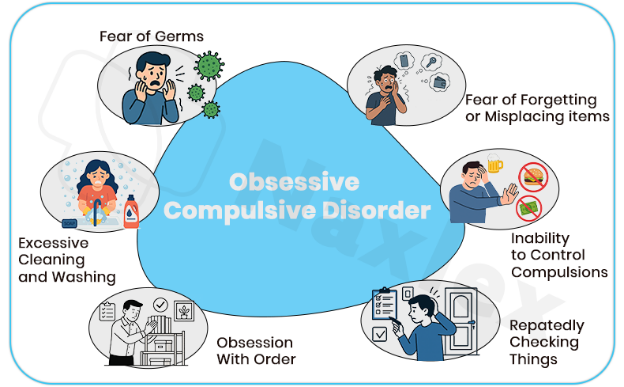
- Common themes include contamination fears, doubts about actions, aggressive or sexual impulses, religious scrupulosity, and symmetry needs.
- Themes are culturally influenced; contamination may involve germs or moral “dirtiness.”
- 90% of OCD patients report multiple themes, with contamination being most prevalent (45-60%).
- Contamination: Fear of dirt, germs, or chemicals leading to avoidance.
- Harm: Intrusive thoughts of harming others or self, despite no intent.
- Symmetry/order: Need for things to be “just right,” linked to perfectionism.
- Forbidden thoughts: Taboo sexual, religious, or blasphemous content causing guilt.
- Contamination obsessions surged during the COVID-19 pandemic, increasing OCD prevalence; nurses screen for exacerbation in public health crises.
1.3 Neurobiological Basis
- Obsessions involve aberrant functioning in the fear circuitry, particularly the orbitofrontal-subcortical loop.
- PET scans reveal hypermetabolism in the caudate nucleus during obsessive states, normalized post-treatment.
- Serotonergic deficits contribute, as low 5-HT levels correlate with symptom severity.
- Glutamatergic hyperactivity in the prefrontal cortex amplifies intrusive thoughts.
- Circuitry dysfunction: Overactivation of cortico-basal ganglia-thalamic loop leads to failure in thought suppression.
- Neurotransmitter roles: Serotonin modulates anxiety; dopamine influences reward in compulsion reinforcement.
- Genetic links: Polymorphisms in COMT and MAOA genes affect catecholamine metabolism, predisposing to obsessional thinking.
Compulsions
- Compulsions are repetitive, purposeful behaviors or mental acts performed in response to obsessions to reduce distress or prevent dreaded events.
- They are not realistically connected to the feared outcome and are excessive.
- Neurologically, compulsions reinforce the obsessive cycle via negative reinforcement, strengthening striatal pathways.
1.1 Purpose of compulsions
- Compulsions are stereotyped responses driven by rigid rules or to neutralize obsessions, often consuming significant time.
- Their purpose is anxiety reduction, but relief is short-lived, perpetuating a vicious cycle.
- Compulsions must be recognized as excessive in most cases.
- Behavioral vs. mental: Physical acts like hand-washing versus covert counting or praying.
- Time consumption: Often exceed one hour daily, impacting productivity.
- Resistance: Attempts to resist increase anxiety, leading to surrender.
- Compulsions provide temporary relief but maintain the disorder, key for explaining exposure therapy rationale.
1.2 Examples of Compulsive Behaviors
- Examples include checking, cleaning/washing, ordering/arranging, hoarding, and mental rituals like repeating phrases.
- Checking compulsions occur in 30% of cases, often linked to doubt obsessions.
- Behaviors can lead to physical harm, such as skin damage from washing.
- Checking: Repeated verification to prevent harm, e.g., ensuring stove is off.
- Washing/cleaning: Ritualistic hand-washing to remove contaminants.
- Counting/repeating: Mental or verbal repetition to “undo” bad thoughts.
Arranging: Aligning objects symmetrically for completeness.
Compulsive Behavior Patterns
- Compulsive behavior patterns are structured, ritualistic sequences evolving into complex routines.
- They are driven by the need to achieve a “just right” feeling, often overt or covert.
- They reflect habit formation in the basal ganglia, where actions become automatized.
1.1 Rituals and Their Impact
- Rituals are elaborate, rule-bound sequences, such as washing hands a specific number of times or following a precise path.
- Impact includes time loss, social isolation, and physical consequences like dermatitis from cleaning.
- Long-term, rituals erode self-efficacy and exacerbate depression.
- Complexity escalation: Rituals become more intricate, increasing impairment.
- Functional interference: Daily activities like work or relationships suffer.
- Emotional toll: Guilt and frustration arise from irrationality awareness.
- Documenting ritual details is crucial, as abrupt interruption causes panic; gradual exposure is key in care plans.
1.2 Differentiation from Other Behaviors
- Compulsions are distinguished from tics (involuntary, as in Tourette’s), stereotypies (in autism), or addictions (pleasure-seeking).
- Compulsions are ego-dystonic and anxiety-driven, unlike habitual behaviors lacking distress.
- Vs. tics: Tics are sudden, non-rhythmic; compulsions are purposeful.
- Vs. impulsivity: In ADHD, actions are spontaneous; compulsions are ritualized.
- Vs. normal rituals: Cultural rituals lack distress; OCD rituals impair functioning.
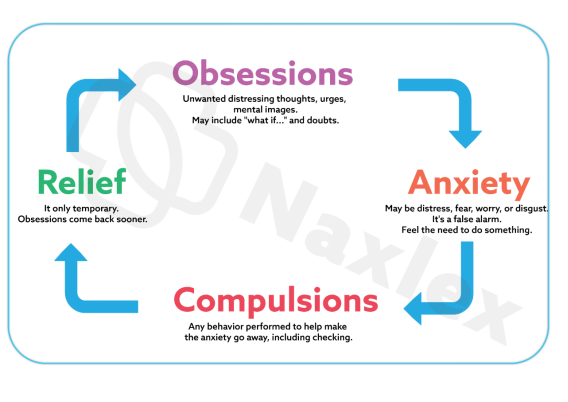
1.3 Cycle of Obsessions and Compulsions
- The cycle begins with an obsession triggering anxiety, followed by compulsion for relief, reinforcing via operant conditioning.
- Breaking this requires therapeutic disruption, as in CBT.
- Trigger: External cue or spontaneous thought.
- Anxiety spike: Physiological arousal.
- Compulsion: Temporary neutralization.
- Reinforcement: Short-term relief perpetuates cycle.
- The obsession-compulsion cycle is maintained by avoidance, guiding nurses to reinforce ERP therapy tolerance.
Related Disorders
- Related disorders are grouped with OCD due to overlapping phenomenology, genetics, and treatment responses.
- They involve repetitive behaviors focusing on body-focused or accumulation issues.
1.1 Body Dysmorphic Disorder
- Body dysmorphic disorder (BDD) involves preoccupation with perceived flaws in appearance that are minor or unobservable.
- Definition: Persistent preoccupation with defects, causing distress or impairment.
- Criteria require repetitive behaviors (e.g., mirror checking) or mental acts (e.g., comparing), not explained by eating disorders, with specifiers for muscle dysmorphia or insight.
- Preoccupation time: At least one hour daily.
- Behaviors: Camouflaging, seeking reassurance, excessive grooming.
- Distress: Leads to social withdrawal or suicidal ideation in 80% of cases.
- Clinical features include high comorbidity with depression (60%) and OCD (30%), with adolescent onset.
- Assessment evaluates delusion-like beliefs and suicide risk (25% attempt rate).
- Common foci: Skin, hair, nose; muscle concerns in males.
- Neurobiology: Visual processing abnormalities in fusiform gyrus.
- Cultural variations: Higher in cosmetic surgery seekers.
- Treatments include SSRIs and CBT focused on appearance beliefs; nurses monitor for dermatological self-harm.
- BDD is underdiagnosed; nurses screen with questions like “Do you worry excessively about your appearance?” to prevent cosmetic procedure traps.
1.2 Hoarding Disorder
- Hoarding disorder entails difficulty discarding possessions, leading to cluttered living spaces and impairment.
- Definition: Accumulation due to perceived need to save items, with distress at discarding.
- Criteria include clutter compromising living areas, not due to other conditions like dementia, with specifiers for acquisition or insight.
- Accumulation: Items of little value, like newspapers or trash.
- Distress: Emotional attachment or fear of needing items.
- Impairment: Health hazards from clutter, e.g., fire risks.
- Features: Onset in teens, worsening with age; 50% have comorbid depression.
- Assessment uses Hoarding Rating Scale, evaluating safety and functionality.
- Demographics: More common in older adults, equal in genders.
- Neurobiology: Frontal lobe deficits in decision-making.
- Complications: Social isolation, eviction risks.
- Treatments include CBT with motivational interviewing; SSRIs are less effective.
- Nursing interventions focus on harm reduction, like organizing sessions.
- Differentiate hoarding from collecting: Hoarding causes distress and clutter; nurses assess home safety for fall risks.
1.3 Trichotillomania (Hair-Pulling Disorder)
- Trichotillomania involves recurrent hair-pulling resulting in hair loss, with failed stop attempts.
- Definition: Repetitive pulling from scalp, eyebrows, or other areas, causing noticeable loss.
- Criteria require tension before pulling or relief after, not due to medical conditions, causing distress.
- Sites: Scalp (75%), eyebrows, eyelashes.
- Behaviors: Automatic (unaware) vs. focused (intentional).
- Prevalence: 1-2%, females predominant.
- Features: Onset in childhood, comorbid with excoriation (50%).
- Assessment examines bald patches and rules out alopecia.
- Psychological: Triggered by stress; may involve eating pulled hair (trichophagia).
- Neurobiology: Reward pathway involvement, similar to addictions.
- Complications: Infections, gastrointestinal issues from ingestion.
- Treatments include habit reversal training and SSRIs; nurses monitor for infections.
- Trichotillomania is body-focused; nurses educate on stress management to avoid misdiagnosis as self-harm.
1.4 Excoriation (Skin-Picking) Disorder
- Excoriation disorder features recurrent skin-picking causing lesions, with unsuccessful stop attempts.
- Definition: Repetitive picking at skin, causing damage.
- Criteria include distress or impairment, not substance-induced, not explained by other disorders.
- Sites: Face, arms, hands.
- Triggers: Boredom, anxiety.
- Duration: Episodes last minutes to hours.
- Features: Comorbid with OCD (40%), females more affected.
- Assessment involves dermatological exam and infection risk evaluation.
- Patterns: Automatic or focused picking.
- Neurobiology: Dopaminergic reinforcement.
- Scarring: Permanent damage common.
- Treatments include CBT, N-acetylcysteine for glutamate modulation; nurses apply wound care.
- Excoriation often co-occurs with acne; nurses promote barrier methods like gloves for habit breaking.
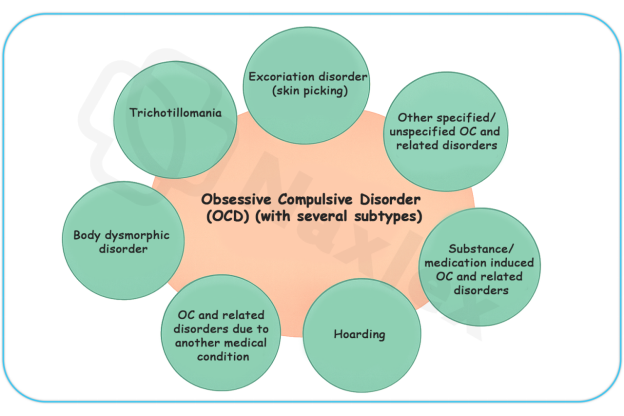
1.5 Substance/Medication-Induced Obsessive-Compulsive and Related Disorder
- Involves OCD-like symptoms from substance intoxication, withdrawal, or medication side effects, like stimulants or corticosteroids.
- Symptoms resolve upon cessation; nurses monitor for underlying vulnerabilities.
- Common agents: Amphetamines induce compulsions; antipsychotics may worsen.
- Assessment: Temporal link to substance use.
1.6 Obsessive-Compulsive and Related Disorder Due to Another Medical Condition
- Symptoms arise from medical issues like brain injury or Sydenham’s chorea.
- Nursing focuses on treating the primary condition.
- Examples: Post-stroke OCD from basal ganglia lesions.
- Diagnosis: Evidence of etiological medical factor.
1.7 Other Specified Obsessive-Compulsive and Related Disorder
- For presentations not meeting full criteria, like body odor concerns (olfactory reference syndrome).
- Subthreshold symptoms with impairment.
1.8 Unspecified Obsessive-Compulsive and Related Disorder
- Used when full criteria are unmet due to insufficient information.
- Temporary diagnosis in emergencies.
- In related disorders, poor insight in BDD predicts cosmetic surgery seeking; nurses advocate for psychiatric evaluation first.
Assessment In Nursing Practice
- Nursing assessment is systematic, incorporating biopsychosocial elements to inform care.
- Begins with building rapport to reduce stigma.
1.1 Screening Tools and Instruments
- Screening uses validated tools like Yale-Brown Obsessive Compulsive Scale (Y-BOCS) for severity, scoring obsessions and compulsions from 0-40.
- Other instruments include Obsessive-Compulsive Inventory (OCI) and Hoarding Rating Scale.
- Y-BOCS: Gold standard, assesses time, interference, distress.
- BDD-YBOCS: Adapted for body dysmorphic disorder.
- Interpretation: Scores >16 indicate moderate OCD needing intervention.
- Use Y-BOCS for initial and follow-up assessments; a 25-35% reduction indicates response, guiding medication adjustments.
1.2 Comprehensive Nursing Assessment
- Covers history, symptom details, functional impact, and comorbidities.
- Physical exam checks for compulsion-related injuries.
- Symptom inquiry: Frequency, triggers, relief methods.
- Mental status: Insight, mood, suicidality.
- Family history: Genetic risks.
1.3 Cultural and Developmental Considerations
- Cultural norms influence symptom expression; e.g., religious obsessions in conservative groups.
- Developmental stages affect presentation: children show more compulsions, elderly more hoarding.
- Cultural sensitivity: Avoid pathologizing cultural rituals.
- Age-specific: Pediatric assessments use play therapy.
Nursing Insights
- In nursing school exams, emphasize that OCD onset peaks bimodally (childhood and early adulthood); nurses screen adolescents during routine health visits, as early intervention reduces suicide risk, elevated 10-fold in untreated OCD.
Nursing Diagnoses And Planning
- Nursing diagnoses are derived from assessment data using frameworks like NANDA-I.
1.1 Common Nursing Diagnoses
- Common diagnoses include Anxiety related to obsessive thoughts, Ineffective Coping due to compulsions, and Impaired Social Interaction from avoidance.
- Anxiety: Evidenced by physiological symptoms.
- Disturbed Thought Processes: From intrusive obsessions.
- Risk for Injury: From skin-picking or hoarding clutter.
1.2 Goal Setting and Outcome Criteria
- Goals are SMART: e.g., Reduce compulsion time by 50% in 4 weeks.
- Outcomes measured by self-reports and scales.
- Short-term: Verbalize understanding of cycle.
- Long-term: Resume occupational functioning.
Interventions And Treatments
- Interventions combine pharmacological, psychotherapeutic, and nursing strategies for symptom reduction and quality of life improvement.
1.1 Pharmacological Interventions
- First-line: SSRIs like fluoxetine (20-80 mg/day), with 40-60% response rate.
- Clomipramine for refractory cases; augmentation with antipsychotics like risperidone.
- Mechanism: Increase serotonin availability.
- Side effects: Sexual dysfunction, weight gain; nurses monitor adherence.
- Onset: 8-12 weeks for full effect.
1.2 Psychotherapeutic Interventions
- Cognitive-behavioral therapy (CBT) challenges dysfunctional beliefs; effective in 70% of cases.
- Cognitive restructuring: Reframe obsessions as harmless.
- Mindfulness: Acceptance and commitment therapy variants.
1.3 Exposure and Response Prevention Therapy
- ERP involves gradual exposure to obsessions without compulsions, habituating to anxiety; 60-85% efficacy.
- Hierarchy building: Rank fears from least to most.
- Sessions: Weekly, with homework.
- Nursing role: Support during distress.
- ERP is superior to medication alone; nurses reinforce homework compliance, as dropout rates are 20-30%.
1.4 Nursing-Specific Interventions
- Nurses provide education, monitor medications, and facilitate support groups.
- Therapeutic communication validates distress without reassurance-seeking.
- Milieu therapy: Structured environments to limit rituals.
- Behavioral contracts: Agree on ritual reduction.
1.5 Multidisciplinary Collaboration
Involves psychiatrists, therapists, social workers; nurses coordinate care.
Complications, Prognosis, And Patient Education
- Complications arise from untreated symptoms; prognosis improves with early intervention.
- Education empowers self-management.
1.1 Potential Complications
- Include chronic depression (50% comorbidity), substance abuse, and physical issues like infections from picking or malnutrition in hoarding.
- Suicidality: 10-17% attempt rate in OCD.
- Occupational loss: Unemployment in 20-30%.
- Family strain: Caregiver burden high.
1.2 Prognostic Factors
- Good prognosis with early treatment, good insight, and no comorbidities.
- Poor prognosis in chronic cases; hoarding subtype has worst outcome.
- Response predictors: Family support, therapy adherence.
- Recovery rates: 50% achieve remission with treatment.
1.3 Patient and Family Education Strategies
- Education covers disorder nature, treatment rationale, and relapse prevention.
- Use teach-back methods.
- Topics: Cycle breaking, medication facts.
- Resources: OCD Foundation materials.
- Family involvement: Avoid enabling compulsions.
- Educate on relapse signs like ritual return; schedule follow-ups, as 30% relapse post-treatment.
Nursing Insights
- A key point for nurses is the biopsychosocial model in OCD etiology; assess for streptococcal history in pediatric cases to rule out PANDAS, potentially altering treatment to immunological interventions.
Summary
- OCD and related disorders involve intrusive obsessions and repetitive compulsions or behaviors, rooted in neurobiological dysregulation.
- Key components include obsessions (intrusive thoughts), compulsions (repetitive acts), and compulsive patterns (ritualized sequences).
- Related disorders like body dysmorphic disorder, hoarding disorder, trichotillomania, and excoriation disorder require tailored assessments.
- Nursing involves screening with Y-BOCS, diagnosing Anxiety, and implementing SSRIs, CBT, and ERP.
- Complications like suicidality require vigilant monitoring; prognosis improves with multidisciplinary care and education.
- These concepts equip nurses for scientific, compassionate care using biopsychosocial approaches.
