
Family Planning
Lessons
- Objectives
- Introduction
- Family Planning Fundamentals
- Hormonal Contraception
- Intrauterine Contraception
- Barrier Methods And Spermicides
- Fertility Awareness–based Methods (Fabms)
- Emergency Contraception
- Permanent Contraception
- Special Populations And Medical Eligibility
- Contraceptive Counseling And Patient Education
- Practice Exercise 1
- Clinical Procedures And Complications
- Practice Excercise 2
- Case-based Nursing Management
- Practice Excercise 3
- Summary
- Comprehensive Questions
Notes Highlighting is available once you sign in. Login Here.
Objectives
• Provide a rigorous, scientifically accurate compendium of modern contraceptive methods, including mechanisms of action, indications, contraindications, effectiveness, side-effect profiles, and practical clinical management.
• Apply WHO/CDC Medical Eligibility Criteria (MEC) to individualized contraceptive selection across diverse clinical scenarios (e.g., postpartum lactation, adolescents, VTE risk, migraines with aura, chronic liver disease).
• Master counseling frameworks that operationalize shared decision-making, motivational interviewing, confidentiality standards, and culturally responsive education.
• Execute safe initiation (“Quick Start”), follow-up, troubleshooting, and complication management for hormonal, intrauterine, barrier, FABMs, emergency, and permanent contraception.
• Integrate dual-protection strategies to reduce unintended pregnancy and sexually transmitted infection (STI) transmission, including partner counseling and referral.
• Prepare for high-stakes examinations and real-world clinical practice via embedded Nursing Insights, case-based pearls, and targeted practice questions.
Introduction
Family planning is a cornerstone of reproductive health, enabling individuals and couples to achieve desired birth spacing and family size while minimizing adverse obstetric and neonatal outcomes. Contraceptive care encompasses biomedical selection of methods, longitudinal safety surveillance, anticipatory guidance regarding side effects, and patient-centered counseling rooted in autonomy and equity. For nurses, mastery of contraceptive pharmacology, device techniques, and the MEC framework is essential to deliver evidence-based, culturally safe care across the reproductive lifespan, including adolescence, the immediate postpartum period, and perimenopause.
Family Planning Fundamentals
1.1 Definitions and Epidemiology
• Family Planning: A comprehensive set of services that permits voluntary prevention, spacing, or timing of pregnancies via contraceptive methods, fertility awareness, or permanent sterilization.
• Unintended Pregnancy: A pregnancy that is mistimed or unwanted at conception; it correlates with delayed prenatal care, maternal morbidity, and adverse neonatal outcomes.
• Global and Regional Patterns:
➤ Contraceptive prevalence and method mix vary by geography, cultural norms, legal frameworks, and health system capacity.
➤ Long-acting reversible contraceptives (LARCs) have increased in uptake due to high effectiveness and minimal adherence burden.
• Public Health Impact:
➤ Effective family planning reduces maternal mortality, preterm birth, and low birth weight by optimizing interpregnancy intervals (ideal ≥18–24 months).
➤ Access barriers include cost, stock-outs, provider bias, restrictive policies, and misinformation.
Nursing Insights
• Always document the client’s reproductive intentions (e.g., “pregnant in the next year: yes/no/unsure”). This single question reframes counseling, aligns method tiers with intentions, and identifies those who would benefit from LARC or permanent options.
• Integrate dual protection counseling whenever STI risk is nonzero; recommend condoms in addition to the chosen contraceptive.
• Screen for intimate partner violence (IPV) and reproductive coercion; discuss discreet methods (e.g., implant, IUD, POPs) and provide safety resources.
1.2 Physiology of Fertility and Reproductive Anatomy
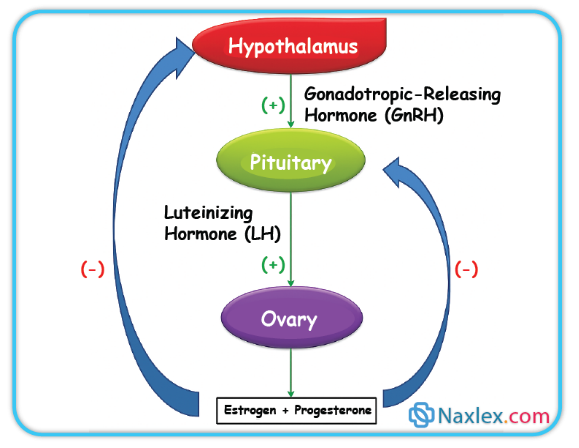
• Hypothalamic–Pituitary–Ovarian (HPO) Axis:
➤ Gonadotropin-releasing hormone (GnRH) pulsatility → pituitary secretion of follicle-stimulating hormone (FSH) and luteinizing hormone (LH).
➤ Folliculogenesis culminates in an LH surge triggering ovulation; luteal progesterone stabilizes endometrium.
• Cervical Mucus Dynamics:
➤ Estrogen-dominant peri-ovulatory mucus becomes abundant, clear, and spinnbarkeit (stretchy), facilitating sperm transport.
➤ Progesterone-dominant luteal mucus is viscous and scant, impeding sperm passage.
• Sperm Transport and Capacitation:
➤ Sperm traverse cervical canal and uterus to the ampulla; capacitation enhances acrosomal reaction for fertilization.
• Implantation Window:
➤ Occurs ~6–10 days post-fertilization; endometrium requires synchronized receptivity (integrins, cytokines, pinopodes).
Nursing Insights
• Clients with irregular cycles may misidentify the fertile window; FABMs require reliable observation training or may be unsuitable.
• Lactation suppresses GnRH, but LAM efficacy requires strict criteria; partial breastfeeding or infant age >6 months markedly reduces protection.
1.3 Mechanisms of Contraception: Biological Targets
• Ovulation Inhibition:
➤ Combined hormonal contraceptives (CHCs) suppress LH surge via negative feedback.
➤ Some progestin-only methods (e.g., implant, DMPA) consistently inhibit ovulation.
• Cervical Mucus Viscosity:
➤ Progestins thicken mucus, reducing sperm penetration (key for POPs and LNG-IUDs).
• Endometrial Effects:
➤ Progestin exposure renders endometrium less receptive to implantation; LNG-IUDs cause glandular atrophy and decidualization.
• Sperm Toxicity/Immobilization:
➤ Copper ions create a spermicidal inflammatory milieu and impair motility (Cu-IUD).
• Mechanical Barrier:
➤ Condoms, diaphragms, caps, and sponges physically prevent sperm from entering the upper genital tract.
1.4 Effectiveness Metrics: Perfect Use vs Typical Use; Pearl Index and Failure Rates
• Perfect Use: Method used consistently and correctly every time.
• Typical Use: Reflects real-world adherence, user error, and discontinuation.
• Pearl Index (PI): Pregnancies per 100 woman-years; lower values indicate higher effectiveness.
• Tiered Counseling:
➤ Tier 1 (Highest efficacy): LARCs (implants, IUDs) and sterilization (failure rate <1%).
➤ Tier 2: CHCs and DMPA (typical failure ~4–7% for CHCs; lower with DMPA adherence).
➤ Tier 3: Barriers, spermicides, FABMs (higher typical-use failure).
Nursing Insights
• When discussing effectiveness, anchor with absolute numbers (“<1 pregnancy per 100 users in a year” for LARCs) and compare with condoms (typical use ~13–18 pregnancies per 100 users/year depending on source). This concreteness improves informed choices.
• Clarify that typical-use failure for user-dependent methods is driven by missed/late doses, ring/patch gaps, or incorrect barrier use; pair with adherence aids (alarms, apps, synchronized refills).
1.5 Determinants of Method Selection: MEC, Comorbidities, Age, Postpartum/Lactation, Medications, Cultural/Legal Factors
• Medical Eligibility Criteria (MEC):
➤ Categorizes safety (1 = no restriction; 4 = unacceptable risk).
➤ Absolute CHC contraindications include migraine with aura, current smoking ≥35 years with ≥15 cigarettes/day, VTE, certain thrombophilias, severe hypertension, ischemic heart disease, stroke, active hepatic disease, and breast cancer.
• Life Stage Considerations:
➤ Adolescents: Favor LARCs for high efficacy and privacy; address confidentiality and STI risk.
➤ Postpartum/Lactating: Avoid estrogen early postpartum due to VTE risk and potential effect on milk supply; POPs, implant, IUDs are preferred.
➤ Perimenopause: Consider VTE risk and comorbidities; non-estrogen options often preferred.
• Medication Interactions:
➤ Enzyme inducers (e.g., rifampin-class, certain anticonvulsants) reduce steroid levels; recommend Cu-IUD, LNG-IUD, or DMPA/implant depending on agent.
• Cultural/Religious and Legal Contexts:
➤ Respect beliefs while providing accurate, unbiased information and alternatives (e.g., FABMs).
• Health Equity:
➤ Proactively mitigate barriers (cost, transport, clinic hours); offer same-day initiation, long refills, and community outreach.
Nursing Insights
• Quick safety screen heuristic: “HEADACHE” mnemonic for CHC red flags: Hypertension, Embolism (VTE), Aura (migraine), Diabetes with vascular disease, Age ≥35 + heavy Cigarettes, Hepatopathy, Estrogen-sensitive malignancy.
• For clients on enzyme-inducing antiepileptics, document a medication–method plan (e.g., implant + condom backup or IUD) and liaise with neurology for possible regimen modification.
Hormonal Contraception
1.1 Combined Hormonal Methods (COCs, Transdermal Patch, Vaginal Ring)
• Mechanism: Ethinyl estradiol (or estradiol valerate) + progestin suppress GnRH/FSH/LH → ovulation inhibition; progestin thickens cervical mucus; endometrium becomes unreceptive.
• Formulations & Regimens:
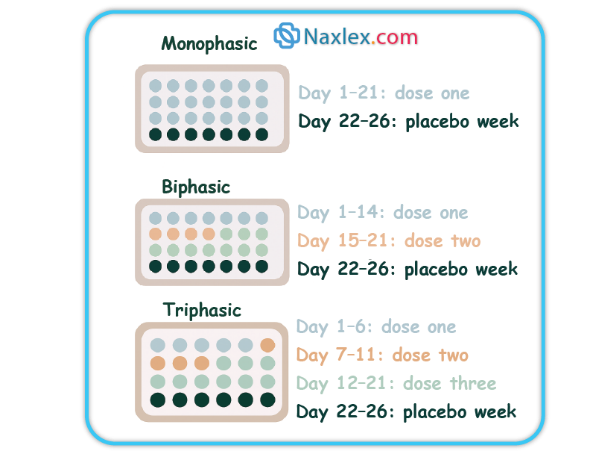
➤ COCs: Monophasic (fixed doses) vs multiphasic; 21/7, 24/4, or extended/continuous cycles.
Weekly application x3 weeks then 1 patch-free week (or continuous); reduced efficacy possible at higher body weight for some products.
➤ Ring: Intravaginal device worn 3 weeks on/1 week off (or continuous).
• Noncontraceptive Benefits:
➤ Reduced dysmenorrhea, menorrhagia, and acne; cycle regulation; reduced risk of endometrial and ovarian cancers with long-term use.
• Contraindications (selected):
➤ Migraine with aura, smoking ≥35y with heavy use, VTE history, major thrombophilia, ischemic heart disease, stroke, severe hypertension, active hepatic disease, estrogen-sensitive cancers, early postpartum.
• Adverse Effects & Management:
➤ Breakthrough bleeding (optimize adherence, consider higher estrogen or different progestin).
➤ Nausea (take with food/at bedtime), breast tenderness, mild BP increase.
➤ Rare: VTE, stroke, MI in high-risk individuals.
• Initiation:
➤ Quick Start if reasonable certainty patient is not pregnant; backup x7 days unless starting within first 5 days of menses.
Nursing Insights
• For clients with migraine with aura, avoid all estrogen-containing methods; prioritize POPs, implant, IUDs, or DMPA.
• Patch adherence issues often stem from detachment; instruct on firm application to clean, dry skin and rotating sites; counsel on replacement if detachment >24 hours.
1.2 Progestin-Only Pills (POPs, “Minipill”)
• Mechanism: Primary—cervical mucus thickening; ovulation suppression in a subset depending on formulation.
• Use Pattern: Same time daily with a narrow window (often ≤3 hours for traditional norethindrone POPs); newer drospirenone POPs allow a slightly longer window per product labeling.

• Candidates: Lactating clients, estrogen contraindications, migraine with aura, smokers ≥35 years.
• Adverse Effects: Irregular spotting/bleeding, amenorrhea in some users.
• Missed Pill Protocol: If late beyond allowed window, take immediately and use backup for specified period (often 48 hours for norethindrone POPs).
Nursing Insights
• Counsel clients to set alarms and keep on-person backup condoms; a single late POP dose can reduce efficacy due to mucus thinning.
1.3 Injectable Progestin (Depot Medroxyprogesterone Acetate, DMPA)
• Dosing: 150 mg IM or 104 mg SC every 12–13 weeks.
• Mechanism: Consistent ovulation suppression, thickened cervical mucus, and endometrial atrophy.
• Benefits: Highly effective, privacy, reduction in dysmenorrhea and endometriosis-related pain; potential seizure threshold benefits.
• Adverse Effects:
➤ Menstrual changes: Irregular bleeding initially, progressing to amenorrhea in many users.
➤ Weight gain in some; delayed return to fertility (median ~9–10 months after last injection).
➤ Bone mineral density (BMD) loss—generally reversible; ensure calcium/vitamin D intake and weight-bearing exercise.
• Considerations:
➤ Good for those who cannot use estrogen or desire infrequent dosing; provide on-time appointment systems.
Nursing Insights
• At initiation, set next injection appointment before discharge and send calendar invites/text reminders. Discuss expected bleeding patterns proactively to reduce discontinuation.
1.4 Contraceptive Implant (Etonogestrel Subdermal Implant)
• Duration: Up to 3 years (some guidelines allow extended use in certain contexts).
Inhibits ovulation and thickens cervical mucus.
• Effectiveness: >99% typical-use; rapid return to fertility on removal.
• Adverse Effects: Irregular bleeding patterns (spotting, amenorrhea, or prolonged bleeding), rare insertion/removal complications, potential bruising.
• Insertion/Removal: Office-based; confirm palpation post-insertion; maintain site dressing per protocol.
Nursing Insights
• For bothersome bleeding, offer short courses of NSAIDs, combined pills (if no contraindication), or tranexamic acid per local protocols; document shared decision and reassess.
1.5 Drug–Drug Interactions and Special Populations
• CYP3A inducers (e.g., rifampin, certain anticonvulsants, St. John’s wort) can reduce steroid levels, particularly impacting COCs, POPs, and emergency levonorgestrel; consider IUDs or DMPA which are less impacted.
• GI malabsorption (e.g., post-bariatric surgery) may reduce oral method effectiveness; prefer non-oral LARC.
• Obesity: Patch efficacy may be lower at higher body weight for some products; LARCs or IUDs avoid weight-based pharmacokinetic concerns.
1.6 Adverse Effects, Contraindications, and Management Algorithms
• Unscheduled Bleeding:
➤ First 3–6 months: expectant management; rule out pregnancy, STIs, and device malposition if severe/persistent.
➤ Targeted therapy: NSAIDs, short CHC course adjunct (if eligible), or method switch.
• Headache, Nausea, Breast Tenderness: Usually self-limited; supportive care; consider progestin type switch for mood/breast symptoms.
• Serious Events: Educate on ACHES warning for CHCs—Abdominal pain (severe), Chest pain/SOB, Headache (severe), Eye problems, Severe leg pain—seek urgent care.
Nursing Insights
• Use standardized bleeding diaries to track patterns and response to interventions; attach to EMR for continuity.
• When switching methods, avoid gaps: overlap or use backup to maintain protection.
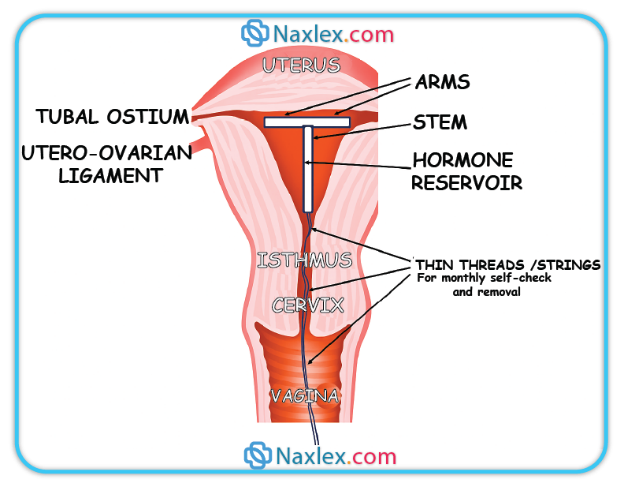
Intrauterine Contraception
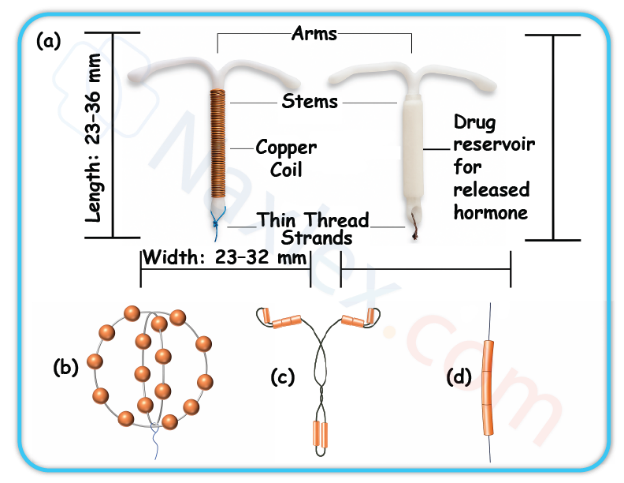
1.1 Copper IUD: Mechanism, Eligibility, Insertion, Adverse Effects
• Mechanism: Copper ions induce sterile endometrial inflammatory response that is spermicidal and prevents fertilization; may impair implantation.
- Effectiveness: >99% with both perfect and typical use; immediate return to fertility on removal.
• Candidates: Desire hormone-free, long-acting, highly effective contraception; suitable as emergency contraception if placed within 5 days of unprotected intercourse.
• Adverse Effects: Heavier/longer menses, dysmenorrhea, especially in first cycles; rare perforation or expulsion.
• Insertion: Screen for pregnancy; STI screening per risk; use aseptic technique; counsel on cramping expectations; trim strings appropriately.
Nursing Insights
• Offer NSAIDs prophylactically before insertion to mitigate cramping; schedule follow-up or PRN visit for heavy bleeding counseling.
1.2 Levonorgestrel IUDs: Types, Doses, Amenorrhea, Noncontraceptive Benefits
• Mechanism: High local progestin levels → thick cervical mucus, endometrial decidualization/atrophy, variable ovulation suppression.
• Variants: Different LNG loads and durations (e.g., 52 mg for up to 5–8 years; lower-dose devices shorter duration per product).
• Benefits: Marked reduction in menstrual blood loss; treatment for heavy menstrual bleeding and dysmenorrhea; protective for endometrial hyperplasia in select contexts.
• Adverse Effects: Irregular bleeding initially, then lighter menses or amenorrhea; rare device complications as above.
Nursing Insights
• Normalize amenorrhea as a benign, expected outcome with LNG-IUDs; emphasize no buildup of blood occurs. Provide written aftercare instructions and when to return.
1.3 IUD Counseling, String Checks, Red Flags, and Complications
• String Check Education: Instruct how to palpate for strings monthly after menses; absence may indicate expulsion or retraction—seek evaluation.
• Red Flags (seek care): Pregnancy symptoms, severe pelvic pain/fever (possible PID), heavy bleeding unresponsive to OTC therapy, suspected expulsion (longer strings or device felt).
• Complications:
➤ Expulsion: Most common in first months; higher after immediate postpartum placement.
➤ Perforation: Rare; risk slightly increased during lactation and early postpartum.
➤ Pregnancy with IUD: If intrauterine pregnancy confirmed, remove IUD if strings visible to reduce adverse outcomes; if ectopic suspected, urgent evaluation.
1.4 Emergency Contraception with IUD
• Copper IUD provides the most effective EC when placed ≤120 hours after unprotected intercourse and offers ongoing contraception.
Nursing Insights
• If pregnancy occurs with IUD in situ, perform prompt location assessment (transvaginal ultrasound, hCG trend). Document counseling on risks and management choices, including continuation vs removal vs pregnancy options.
Barrier Methods And Spermicides
1.1 External (Male) and Internal (Female) Condoms
• External (Male) Condoms:
➤ Constructed of latex, polyurethane, or polyisoprene; a few available in lamb cecum (not protective against STIs).
➤ Mechanism: Physical barrier preventing semen from entering the vagina; latex/polyurethane types provide substantial protection against many STIs including HIV.
➤ Efficacy: Typical use ~82–87% (13–18 pregnancies per 100 women/year); perfect use ~98%.
➤ Use Considerations:
◆ Check expiration date and package integrity.
◆ Apply before any genital contact.
◆ Leave space at tip for semen collection; remove promptly after ejaculation, holding base to prevent slippage.
◆ Avoid oil-based lubricants with latex.
• Internal (Female) Condoms:
➤ Made from nitrile; inserted into vagina prior to intercourse; inner ring anchors near cervix, outer ring remains external.
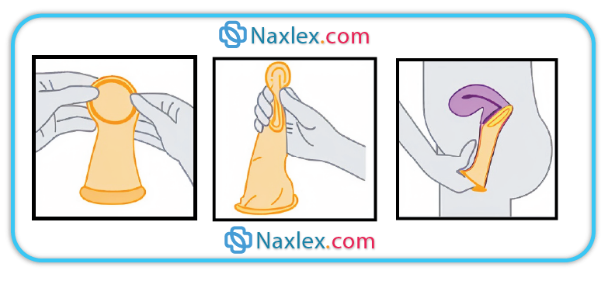
➤ Efficacy: Similar to male condoms with typical use.
➤ Advantages: Female-controlled, may be inserted up to 8 hours before intercourse, provides some protection against STIs.
Nursing Insights
• Demonstrate condom application on a model during counseling to ensure correct use—incorrect technique is a leading cause of barrier method failure.
• Always counsel to use a new condom for each act of intercourse and to store in a cool, dry place (avoid wallets or glove compartments where heat and friction degrade material).
1.2 Diaphragm, Cervical Cap, Contraceptive Sponge
• Diaphragm:
➤ Dome-shaped silicone cup used with spermicide; covers cervix to block sperm entry.
➤ Efficacy: Typical use ~88%; must remain in place ≥6 hours after intercourse but ≤24 hours.
➤ Fitting: Requires prescription and fitting by trained provider; must be refitted after childbirth or ≥10 lb weight change.
• Cervical Cap:
➤ Smaller silicone cup; fits tightly over cervix; used with spermicide.
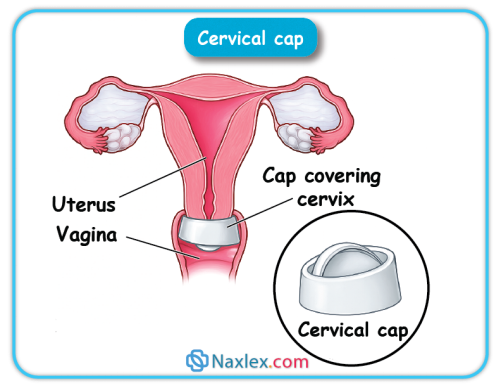
in place up to 48 hours; efficacy lower in parous women.
• Contraceptive Sponge:
➤ Polyurethane device containing nonoxynol-9 spermicide; moistened with water before use; provides up to 24 hours protection regardless of frequency of intercourse.
Nursing Insights
• For diaphragms and caps, emphasize reapplication of spermicide for repeat acts of intercourse without removal.
• Avoid use during menstruation or in women with recurrent urinary tract infections due to increased infection risk.
1.3 Spermicides and Lubricants
• Spermicides:
➤ Nonoxynol-9 most common; immobilizes and kills sperm; available as gels, foams, films, suppositories.
➤ Efficacy as sole method is low (~72% typical use); best used with barriers.
➤ Frequent use (>2/day) may irritate mucosa and increase HIV transmission risk in high-prevalence populations.
• Lubricants:
➤ Water-based and silicone-based safe with latex; oil-based degrade latex.
➤ Can enhance comfort and reduce condom breakage risk if appropriate type is chosen.
Fertility Awareness–based Methods (Fabms)
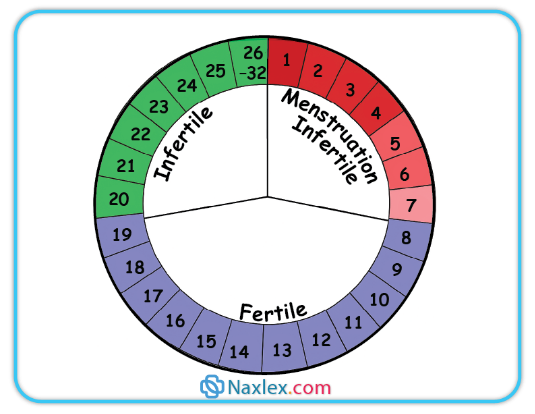
1.1 Calendar/Standard Days Method
• Based on menstrual cycle length; identifies fertile window (Day 8–19 for cycles 26–32 days).
• Requires daily charting; avoid unprotected intercourse during fertile window.
1.2 Cervical
Mucus (Billings) Method
• Daily assessment of mucus characteristics; ovulatory mucus is clear, stretchy (“spinnbarkeit”), slippery.
• Requires abstinence or barrier use during fertile mucus days.

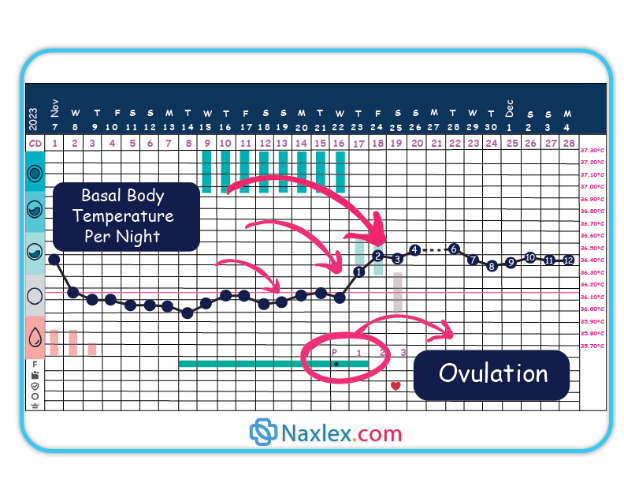
1.2 Basal Body
Temperature (BBT) Method
• Daily temperature upon waking; slight rise (~0.3–0.5°C) after ovulation due to progesterone.
• Fertile window ends 3 days after temperature rise; sensitive to illness, alcohol, poor sleep.
1.4 Symptothermal Method
• Combines BBT, cervical mucus, and other ovulation signs (e.g., mittelschmerz, cervical position).
• More effective than single-indicator methods.
1.5 Lactational Amenorrhea Method (LAM)
• Effective if:
➤ Infant <6 months old.
➤ Exclusive or near-exclusive breastfeeding on demand, day and night.
➤ Amenorrheic.
Nursing Insights
• FABMs require high motivation, consistent daily tracking, and partner cooperation; unsuitable for clients with irregular cycles.
• Illness, stress, or postpartum changes may alter fertility signs, leading to reduced reliability.
Emergency Contraception
1.1 Levonorgestrel Regimens
• Single-dose 1.5 mg or two doses of 0.75 mg 12 hours apart; available OTC in many settings.
• Most effective when taken within 72 hours but may have some efficacy up to 120 hours.
• Mechanism: Delays ovulation if not yet occurred.
Add ectopic pregnancy risk
1.2 Ulipristal Acetate
• Selective progesterone receptor modulator; effective up to 120 hours after unprotected intercourse; prescription required in many places.
• Superior efficacy to levonorgestrel in later part of 5-day window.
• Should not restart hormonal contraception until 5 days after use due to possible interaction.
1.3 Copper IUD as Emergency Contraception
• Most effective EC method; insert within 5 days of unprotected intercourse; provides ongoing contraception.
• Consider for clients at high risk of repeat unprotected sex and those wanting long-term contraception.
1.4 Counseling and Follow-Up After EC
• Warn about possible menstrual changes; advise pregnancy test if no withdrawal bleed within 3 weeks.
• Provide ongoing contraception initiation to prevent future unprotected episodes.
Nursing Insights
• EC does not terminate an established pregnancy—important for patient education to address misconceptions.
• Always use EC counseling as an opportunity to discuss and initiate a regular, reliable contraceptive method.
Permanent Contraception
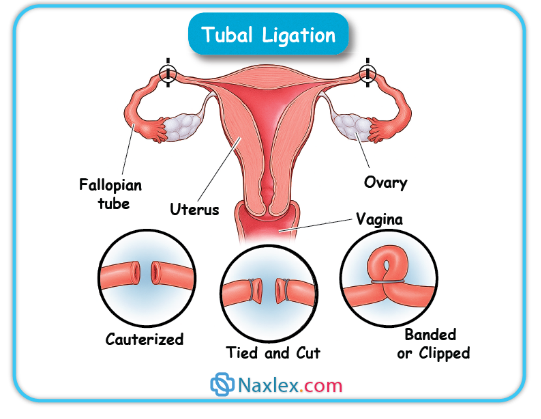
1.1 Female Sterilization (Tubal Ligation/Salpingectomy)
• Mechanism: Occlusion, ligation, cauterization, or complete removal (salpingectomy) of the fallopian tubes to prevent sperm–oocyte meeting.
• Effectiveness: >99% in preventing pregnancy; failure rate ~0.5% in 10 years.
• Timing: Interval (nonpregnant state), postpartum (within 24–48 hours after delivery), or postabortion.
Advantages: Permanent, no ongoing maintenance, no hormonal exposure.
• Disadvantages: Requires surgery; carries anesthesia and surgical risks; regret possible, especially in women <30 years.
• Noncontraceptive Benefits: Bilateral salpingectomy may reduce ovarian cancer risk.
Nursing Insights
• Counsel on permanence—emphasize that reversal is not always possible or successful.
• Screen for ambivalence and external pressure; regret rates higher in younger patients and those with few children at time of procedure.
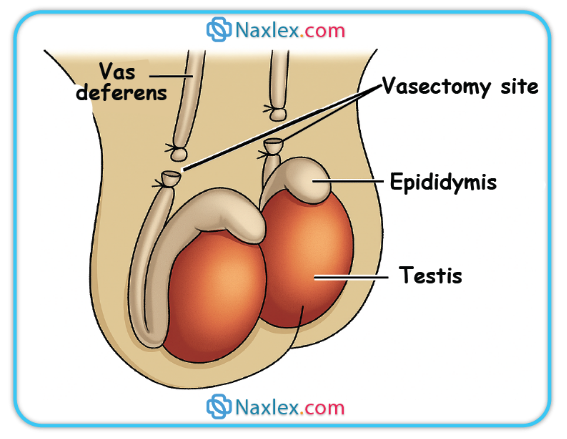
1.2 Male Sterilization (Vasectomy)
• Mechanism: Ligation or cauterization of vas deferens bilaterally to block sperm transport from testes to urethra.
• Effectiveness: >99% after azoospermia confirmed by semen analysis.
• Post-Procedure:
➤ Not immediately effective—backup contraception required until 1–2 semen analyses confirm no sperm (usually at 8–16 weeks or after 20 ejaculations).
Advantages: Minor outpatient procedure; safer and less invasive than female sterilization.
• Disadvantages: Requires surgical access; small risk of chronic testicular pain; not protective against STIs.
Nursing Insights
• Many failures occur because couples stop using backup contraception before azoospermia is documented—schedule and emphasize follow-up semen analysis.
1.3 Regret, Failure, and Pre-Operative Counseling
• Regret Rates: Higher in those sterilized at a young age, during emotional distress, or under partner/family pressure.
• Failure: Rare, often due to technical error or recanalization.
• Pre-Operative Counseling:
➤ Discuss all reversible methods before sterilization.
➤ Obtain informed consent; document patient understanding and voluntary choice.
Special Populations And Medical Eligibility
1.1 Postpartum and Lactating Clients
• <21 days postpartum: CHCs contraindicated due to elevated VTE risk; progestin-only methods and non-hormonal methods are acceptable.
• Lactation: Estrogen can potentially decrease milk volume if started before lactation established; progestin-only and non-hormonal methods preferred.
1.2 Adolescents
• LARCs recommended as first-line by major organizations due to high efficacy and continuation rates.
• Emphasize confidentiality, STI prevention, and consent laws.
1.3 Perimenopause and ≥40 Years
• Fertility declines but persists; contraception recommended until menopause confirmed (12 months amenorrhea).
• CHCs may aid cycle regulation and vasomotor symptoms in healthy nonsmokers without contraindications.
1.4 Comorbidities
• Hypertension: Avoid CHCs in uncontrolled cases; progestin-only or non-hormonal preferred.
• VTE/Migraine with Aura: Avoid estrogen-containing methods.
• Liver Disease: Hormonal methods may be contraindicated in severe hepatic dysfunction.
• Diabetes: With vascular disease, avoid CHCs.
1.5 Enzyme-Inducing Medications
• Reduce efficacy of many hormonal methods except DMPA and IUDs.
• Counsel on backup methods or switching.
1.6 Cultural Sensitivity and Health Equity
• Assess beliefs, address myths respectfully, provide information in patient’s preferred language, and consider access barriers.
Nursing Insights
• Always cross-check patient’s health status against WHO/CDC Medical Eligibility Criteria before initiating a method.
• When working with adolescents, use developmentally appropriate language and ensure the encounter supports autonomy.
Contraceptive Counseling And Patient Education
1.1 Counseling Frameworks: Shared Decision-Making & Motivational Interviewing
• Explore patient values, preferences, reproductive goals.
• Provide unbiased, evidence-based information on all methods.
• Encourage patient participation and confirm understanding.
1.2 WHO/CDC MEC, Quick Start, and Follow-Up
• Use MEC to screen for contraindications.
• Quick Start method: Initiate contraception on day of visit if reasonably certain patient is not pregnant; backup needed for some methods.
• Schedule follow-up to assess satisfaction, side effects, and adherence.
1.3 Documentation, Informed Consent, Legal/Ethical Considerations
• Record counseling, method chosen, and patient’s consent.
• Be aware of laws regarding minors and contraception, spousal consent, and method-specific regulations.
1.4 Public Health Impact and Socioeconomic Benefits
• Reduces unintended pregnancies, maternal mortality, and abortion rates.
• Supports education and workforce participation.
Nursing Insights
• Always provide written materials and referral resources.
• Avoid coercive language—support patient autonomy.
• Be prepared to address myths (e.g., “IUDs cause infertility”) with factual information.
Clinical Procedures And Complications
1.1 Method Initiation Protocols and Timing
• Quick Start Protocol:
➤ Initiate contraception on the same day of the visit if reasonably certain the patient is not pregnant.
➤ Backup contraception required for some methods (e.g., CHCs, POPs) for a specified number of days unless initiated within first 5 days of menses.
• First-Day Start:
➤ Begin on day 1 of menstrual bleeding; immediate contraceptive protection for most hormonal methods.
• Sunday Start:
➤ Begin on the first Sunday after menstruation begins; designed to minimize weekend bleeding but requires backup for the first 7 days.
• Postpartum Start:
➤ Progestin-only methods and non-hormonal methods may be initiated immediately postpartum.
➤ CHCs delayed to ≥21 days postpartum if not breastfeeding, ≥42 days if breastfeeding and no VTE risk factors.
• Postabortion Start:
➤ Most methods can be initiated immediately following abortion or pregnancy loss, unless contraindications exist.
Nursing Insights
• For Quick Start, document last menstrual period, recent unprotected intercourse, and negative pregnancy test if performed; counsel on need for follow-up pregnancy test if there is any uncertainty.
• When counseling postpartum patients, ensure consideration of lactation impact and VTE risk timing.
1.2 Managing Side Effects and Complications
• Hormonal Methods:
➤ Breakthrough Bleeding: Often resolves after 3–6 months; may require dose adjustment or different progestin formulation.
➤ Nausea: Recommend taking with food or at bedtime.
➤ Weight Changes: Provide counseling on diet and exercise; assess for fluid retention.
➤ Mood Changes: Evaluate for history of mood disorders; consider progestin type change or non-hormonal method.
• IUD Complications:
➤ Expulsion: Educate on string check; most common in the first year.
➤ Perforation: Rare; usually occurs at insertion.
➤ Infection: Risk highest in first 20 days post-insertion; screen for STIs as indicated.
Nursing Insights
• Bleeding diaries are a practical tool to evaluate severity and impact of abnormal uterine bleeding on quality of life; adjust method based on pattern.
1.3 Suspected Pregnancy and Contraceptive Failure
• Assess Method Use: Check adherence, storage, timing, and any potential drug interactions.
• Testing: Confirm pregnancy with serum or urine hCG.
• Management:
➤ Hormonal Methods: Discontinue if pregnancy confirmed; no evidence of teratogenicity but unnecessary exposure avoided.
➤ IUD: If pregnant, remove IUD if strings visible to reduce risk of adverse outcomes.
1.4 STI Screening and Dual Protection Strategies
• Screening:
➤ Conduct based on risk assessment and CDC guidelines.
➤ Offer concurrent STI testing when initiating contraceptives.
• Dual Protection:
➤ Recommend condom use in addition to primary contraceptive for STI prevention, particularly in high-risk populations.
Nursing Insights
• Always emphasize that most contraceptive methods do not protect against STIs—condoms are essential for STI prevention in at-risk individuals.
Case-based Nursing Management
1.1 Adolescent First-Visit Contraception
• Scenario: 16-year-old seeking contraception, concerned about confidentiality.
• Approach: Assess sexual history, provide STI counseling, offer LARC as first-line, ensure privacy, clarify consent laws.
1.2 Postpartum, Lactation-Compatible Choices
• Scenario: 3 weeks postpartum, exclusively breastfeeding.
• Approach: Offer progestin-only pills, implant, or IUD; avoid CHCs until ≥6 weeks due to lactation and VTE risk.
1.3 Contraception with VTE/Migraine Risks
• Scenario: 30-year-old smoker with migraine with aura.
• Approach: Avoid estrogen-containing methods; recommend progestin-only or non-hormonal.
1.4 Irregular Cycles and PCOS
• Scenario: 25-year-old with oligomenorrhea and hyperandrogenism.
• Approach: CHCs for cycle regulation and androgen reduction if no contraindication; counsel on metabolic risk.
1.5 Postabortion Contraceptive Initiation
• Scenario: Client desires IUD after first-trimester abortion.
• Approach: Same-day IUD insertion if no infection; provide EC counseling for future prevention if indicated.
Nursing Insights
• Each scenario should be documented with method offered, rationale, patient preference, and informed consent.
• Always incorporate risk reduction for STIs in counseling, even if primary contraceptive method is non-barrier.
Summary
Family planning is an essential component of reproductive healthcare, enabling individuals and couples to achieve their desired timing and spacing of pregnancies while reducing unintended pregnancies and adverse maternal–infant outcomes. Contraceptive methods vary in mechanism, efficacy, reversibility, and suitability depending on patient-specific factors such as age, comorbidities, postpartum status, lactation, medication use, and cultural considerations.
Hormonal methods—including combined estrogen–progestin formulations (COCs, patch, ring) and progestin-only options (POPs, DMPA, implant)—primarily function by suppressing ovulation, thickening cervical mucus, and altering the endometrium. Non-hormonal intrauterine devices, particularly the copper IUD, act through a spermicidal inflammatory response. Levonorgestrel IUDs provide both high contraceptive efficacy and noncontraceptive benefits, such as menstrual reduction and treatment of heavy bleeding.
Barrier methods (male/female condoms, diaphragm, cervical cap, sponge) prevent sperm entry and may also provide STI protection, especially condoms. Fertility Awareness–Based Methods (FABMs) rely on recognition of fertile signs but require highly motivated, disciplined users. Emergency contraception options include levonorgestrel, ulipristal acetate, and copper IUD insertion—the latter being the most effective and longest-lasting solution.
Permanent methods (tubal ligation, vasectomy) offer highly effective contraception but require thorough counseling on irreversibility and follow-up, such as post-vasectomy semen analysis. Special populations—including adolescents, postpartum and lactating individuals, and those with medical comorbidities—require tailored method selection using the WHO/CDC Medical Eligibility Criteria to maximize safety and efficacy.
Effective contraceptive counseling hinges on shared decision-making, unbiased information delivery, cultural sensitivity, and informed consent. Nurses play a pivotal role in initiating, managing, and troubleshooting contraceptive methods, addressing side effects, reinforcing dual protection for STI prevention, and promoting health equity in reproductive care.
