
Parkinson’s Disease
Lessons
- Complications And Prognosis
- Objectives
- Definition And Overview
- Etiology
- Pathophysiology Of Parkinson’s Disease
- Clinical Manifestations
- Practice Exercise 1
- Diagnostic Process And Evaluation
- Practice Exercise 2
- Nursing Care Plan
- Patient And Family Education And Support
- Practice Exercise 3
- Summary
- Comprehensive Questions
Notes Highlighting is available once you sign in. Login Here.
Complications And Prognosis
PD is chronic and progressive; symptoms worsen over time. Not directly fatal, but complications increase morbidity/mortality.
Complications
- Depression and Dementia: Common, especially in advanced stages; increased confusion, hallucinations, agitation.
- Laryngeal Dysfunction and Aspiration Pneumonia: Dysphagia leads to aspiration, major cause of illness/death. Weak cough reflex.
- Autonomic Dysfunction: Orthostatic hypotension (falls risk), urinary retention, erectile dysfunction.
- Falls: Increased risk due to balance problems, gait issues, orthostatic hypotension. Leading cause of ER visits/hospitalizations.
- Pressure Ulcers: Due to immobility; risk of infection/sepsis.
- Kyphosis: Flexed posture can lead to spinal curvature, cardiopulmonary impairment.
- Other Infections and Frailty: Increased susceptibility to infections, reduced resilience to new medical problems. Hospitalization risks (medication disruption, increased immobility, UTIs).
Disease Progression and Long-Term Prognosis
PD is progressive, but progression rate varies. No way to predict individual course. Advanced PD (longer duration, higher Hoehn and Yahr stage, cognitive dysfunction, hallucinations, comorbidities) linked to increased mortality risk. Patients typically succumb to complications (pneumonia, sepsis from ulcers, fall complications) on top of increasing disability/frailty. Proactive management minimizes risks.
Objectives
- Define Parkinson’s disease and describe its underlying pathophysiology, including the role of dopamine and basal ganglia dysfunction.
- Identify the cardinal motor symptoms of Parkinson’s disease: bradykinesia, resting tremor, rigidity, and postural instability.
- Describe common non-motor symptoms of Parkinson’s disease, including cognitive changes, mood disturbances, sleep disorders, and autonomic dysfunction.
- List the risk factors for developing Parkinson’s disease, including age, sex, environmental exposures, and genetic predisposition.
- Explain the clinical diagnosis process, including history-taking, physical exam findings, and the role of response to dopaminergic therapy.
- Differentiate Parkinson’s disease from similar disorders, such as essential tremor, Parkinson-plus syndromes, and normal pressure hydrocephalus.
- Outline pharmacologic treatment options, including levodopa-carbidopa, dopamine agonists, MAO-B inhibitors, and their side effects.
- Describe non-pharmacologic management strategies, including physical therapy, occupational therapy, nutrition, and patient/family education.
Definition And Overview
Parkinson's disease (PD) is a progressive neurodegenerative disorder characterized by bradykinesia (slow movement) and at least one of the following: resting tremor or rigidity. Non-motor symptoms like loss of smell, sleep issues (e.g., REM behavior disorder), depression, drooling, and constipation often precede motor symptoms. Pathologically, PD involves the loss of dopamine-producing neurons in the substantia nigra and the presence of Lewy bodies (abnormal alpha-synuclein protein aggregates). This broad symptom profile highlights PD as a complex systemic disorder.
Etiology
Most PD cases are idiopathic, resulting from a complex interplay of genetics and environment.
Genetic Factors:
- GBA (GBA1): Most common (5-10% of PD); a risk factor, not causative. Associated with earlier onset, faster dementia progression, greater motor difficulties.
- PRKN (Parkin): Most common cause of young-onset PD (<50). Associated with early bradykinesia/rigidity, less dementia, good levodopa response.
- PINK1: Associated with early bradykinesia/rigidity, less non-motor symptoms, slow progression, good levodopa response.
Environmental Risk Factors:
- Pesticides/Herbicides (e.g., paraquat, rotenone).
- Solvents (e.g., trichloroethylene).
- Polychlorinated Biphenyls (PCBs).
- MPTP (synthetic neurotoxin).
- Heavy Metals (e.g., manganese, lead).
- Head Injury (with altered consciousness).
Protective Factors:
- Caffeine consumption.
- Higher uric acid levels.
- Regular NSAID use.
- Cigarette smoking.
- Statin use.
- Higher Vitamin D levels.
- Increased physical activity earlier in life.
Pathophysiology Of Parkinson’s Disease
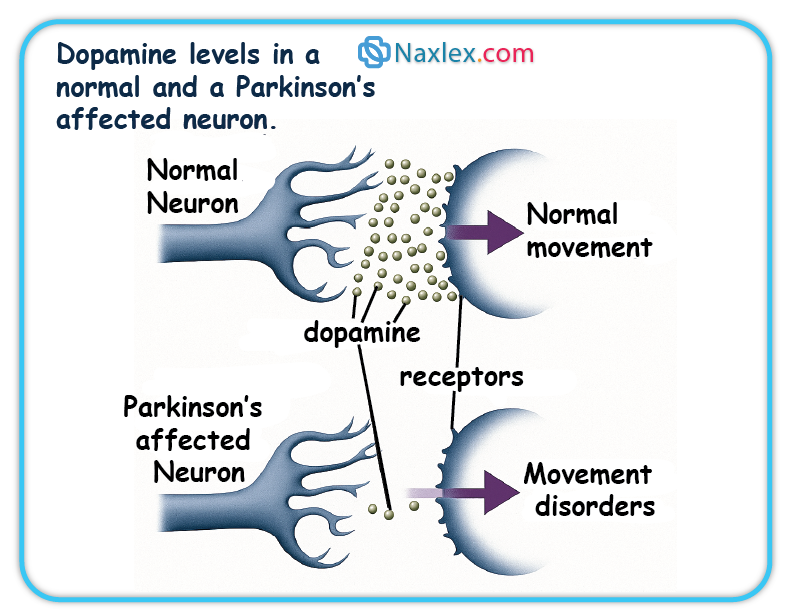
Neurotransmitter Imbalance
PD's core mechanism is the progressive death of dopamine-producing neurons in the substantia nigra. This dopamine deficiency impairs nerve cell communication, leading to motor symptoms. The brain may compensate with high glutamate levels. Treatment aims to restore dopamine activity.
 Alpha-Synuclein Aggregation and Lewy Bodies
Alpha-Synuclein Aggregation and Lewy Bodies
Lewy bodies (LB) and Lewy neurites (LN) are abnormal protein aggregates in neurons, primarily composed of misfolded alpha-synuclein. These misfolded proteins aggregate into filaments, forming LBs, which disrupt cell function and contribute to neuronal death. Early oligomeric forms of alpha-synuclein are thought to be most neurotoxic. LBs are found in various brain regions, correlating with both motor and non-motor symptoms.
Basal Ganglia Dysfunction
PD is a disorder of the basal ganglia, brain nuclei vital for movement control. Loss of dopaminergic neurons in the substantia nigra reduces dopamine in the striatum, disrupting basal ganglia circuitry. This imbalance leads to overactivity in some pathways and underactivity in others, causing bradykinesia, rigidity, and tremor.
Clinical Manifestations
PD symptoms are motor and non-motor, often starting insidiously and asymmetrically.
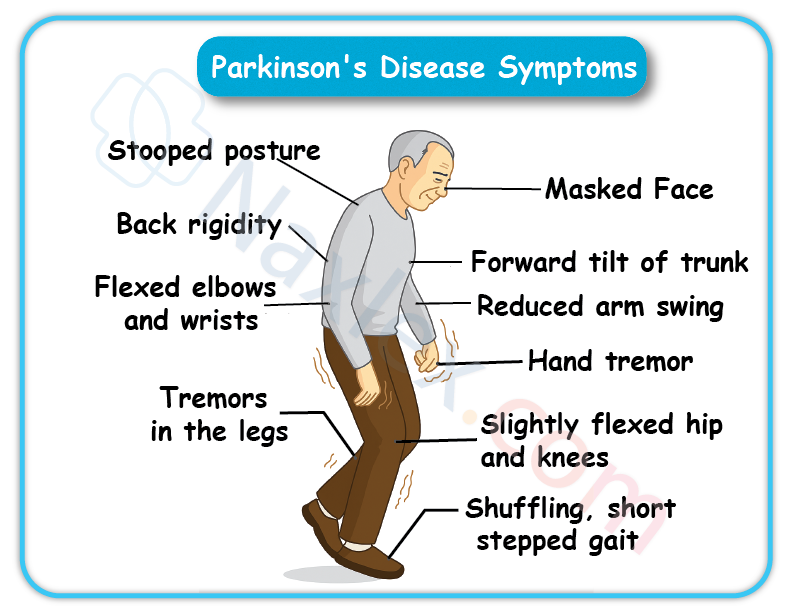
Motor Symptoms (TRAP)
- Tremor: Often initial, resting tremor (e.g., "pill-rolling"), diminishes with action.
- Rigidity: Increased muscle stiffness, resistance to passive movement ("lead pipe" or "cogwheel"), reduced arm swing.
- Akinesia (Slowness of Movement): Core feature; difficulty initiating/executing movements, slow daily tasks, reduced reaction time, micrographia (small handwriting).
- Postural (Gait) Disturbance: Later symptom; flexed posture, shuffling steps (festination), reduced arm swing, "freezing of gait," turning "en bloc."
Non-Motor Symptoms
Often precede motor symptoms and impact quality of life.
- Loss of smell (anosmia).
- Sleep dysfunction (e.g., REM behavior disorder, daytime sleepiness).
- Mood disorders (depression, anxiety, apathy).
- Excess salivation (drooling).
- Constipation.
- Autonomic dysfunction (orthostatic hypotension, dysphagia, urinary issues, sexual dysfunction).
- Dementia (cognitive decline in advanced stages).
 Stages of Parkinson's Disease (Hoehn and Yahr Scale)
Stages of Parkinson's Disease (Hoehn and Yahr Scale)
- Stage 0: No signs.
- Stage 1: Unilateral involvement.
- Stage 1.5: Unilateral plus axial involvement.
- Stage 2: Bilateral disease, no balance impairment.
- Stage 2.5: Mild bilateral, recovers on pull test.
- Stage 3: Mild to moderate bilateral, some postural instability, physically independent.
- Stage 4: Severe disability, still walks/stands unassisted.
- Stage 5: Wheelchair-bound or bedridden unless aided.
Diagnostic Process And Evaluation
Diagnosis is primarily clinical, based on history and neurological exam.
Clinical Diagnosis
Based on bradykinesia plus resting tremor or rigidity, often with asymmetric onset.
Exclusion of Other Conditions
Rule out drug-induced parkinsonism (e.g., from antipsychotics), other alpha-synucleinopathies (Lewy body dementia, multiple system atrophy), tauopathies (progressive supranuclear palsy), and other conditions (essential tremor, Huntington chorea, normal pressure hydrocephalus).
Role of Imaging Studies
- MRI: Excludes other conditions (stroke, tumors, hydrocephalus).
- DaTscan (Dopamine Transporter Scan): Identifies loss of dopaminergic neurons in striatum. Useful to distinguish PD from essential tremor, drug-induced parkinsonism, and vascular parkinsonism when clinical diagnosis is unclear. Cannot distinguish PD from other parkinsonian syndromes (PSP, CBD, MSA). Not for monitoring progression.
Response to Levodopa Treatment
A clear, sustained positive response to levodopa strongly supports a PD diagnosis.
Rating Scales
- Unified Parkinson Disease Rating Scale (UPDRS): Comprehensive assessment of motor and non-motor symptoms.
- Hoehn and Yahr Staging: Global measure of disease progression.
Pharmacological Management
Pharmacology is key for symptom control, not cure. Most patients need combination therapy. Response may weaken over time. Adherence is crucial; abrupt stopping can be dangerous.
Drug Classes, Mechanisms, Side Effects, and Nursing Implications
Levodopa/Carbidopa
- Mechanism: Levodopa (dopamine precursor) crosses BBB, converts to dopamine. Carbidopa prevents peripheral breakdown, increasing brain availability and reducing GI side effects. Most effective for bradykinesia, rigidity, tremor.
- Side Effects: Nausea/vomiting, dizziness, postural hypotension, headache, daytime sleepiness, confusion, hallucinations, dyskinesias, "on-off" episodes. Harmless dark urine/sweat. Possible melanoma risk.
- Nursing Implications: Start low, full effect up to 6 months. Monitor "on-off" and dyskinesias. Assess for orthostatic hypotension, psychosis. Avoid high-protein foods. Do not stop abruptly (risk of parkinsonism hyperpyrexia syndrome). Avoid alcohol, reserpine, pyridoxine (B6), phenothiazine.
Dopamine Agonists
- Mechanism: Directly stimulate dopamine receptors, mimicking dopamine. Used early to delay levodopa, or as adjuncts for motor fluctuations.
- Side Effects: Hallucinations, delusions, confusion, drowsiness, sudden sleep attacks, impulsive behaviors, nausea/vomiting, dry mouth, orthostatic hypotension.
- Nursing Implications: Start low, titrate gradually. Monitor for hallucinations, confusion, impulsive behaviors (especially in elderly). Advise against driving if sudden sleepiness occurs. Do not stop abruptly (risk of withdrawal syndrome).
MAO-B Inhibitors
- Mechanism: Block MAO-B enzyme, increasing dopamine availability in brain. Used alone in early PD or as add-on to levodopa to reduce "off" time.
- Side Effects: Heartburn, nausea, dry mouth, dizziness, insomnia, headaches, confusion, hallucinations. May worsen dyskinesia. Risk of hypertensive crisis with tyramine-rich foods or certain antidepressants.
- Nursing Implications: Full effect in 2-3 weeks. Monitor for dyskinesia (may need levodopa dose reduction). Avoid certain antidepressants, decongestants. Educate on tyramine-rich foods.
COMT Inhibitors
- Mechanism: Block COMT enzyme, preventing levodopa breakdown in periphery, extending levodopa's half-life and "on" time. Always used with levodopa.
- Side Effects: Diarrhea, dyskinesia (may worsen), confusion, hallucinations, dizziness, falls. Harmless reddish-orange urine. Tolcapone has rare liver damage risk (requires monitoring).
- Nursing Implications: Always take with levodopa. Levodopa dose may need reduction. Monitor for dyskinesia, diarrhea. For tolcapone, strict liver function monitoring. Avoid iron supplements concurrently with entacapone.
Anticholinergics
- Mechanism: Block acetylcholine, reducing tremor and rigidity. Minimal effect on bradykinesia/postural instability. Can reduce drooling.
- Side Effects: Cognitive deficits, confusion, memory impairment, sedation, delirium, hallucinations (especially in elderly). Dry mouth, blurred vision, constipation, urinary retention.
- Nursing Implications: Used for younger patients, primarily for tremor/dystonia; avoid in those over 70. Start low, titrate gradually. Monitor for cognitive side effects. Manage dry mouth, constipation, urinary retention. Contraindicated in narrow-angle glaucoma, myasthenia gravis, severe ulcerative colitis.
VI. Non-Pharmacological Management and Surgical Interventions
Holistic management includes therapies and, for select patients, surgery.
Therapies
- Physical Therapy (PT): Improves gait, balance, strength, flexibility. Includes cardiorespiratory, resistance, flexibility, gait/balance training. Teaches movement strategies (rocking, large steps, arm swing).
- Occupational Therapy (OT): Maximizes fine motor skills, adapts ADLs, provides adaptive equipment.
- Speech Therapy: Addresses communication (dysarthria, hypophonia) and swallowing (dysphagia). Teaches facial/tongue exercises, voice amplification, safe swallowing.
- Complementary Therapies: Yoga, Tai Chi, Qigong, acupuncture, massage, art/music therapy, meditation. May help with symptoms and well-being.
Surgical Interventions
For advanced motor complications not controlled by medication.
Deep Brain Stimulation (DBS)
- Description: Electrodes implanted in specific brain areas (STN, GPi) connected to a chest neurostimulator. Delivers continuous electrical impulses to modulate abnormal brain activity. Does not damage brain tissue.
- Indications: Disabling tremors, significant motor fluctuations ("on-off"), medication-induced dyskinesias, good levodopa response but with side effects. PD symptoms for at least 4 years.
- Benefits: Significant symptom reduction, reduced medication dosages, decreased dyskinesia. Benefits last at least 5 years. Reversible and adjustable.
- Risks/Complications: Small risk of infection, stroke, bleeding, seizure. Post-op: reduced speech clarity, subtle word-finding issues, cognitive decline (if pre-existing).
- Nursing Care:
- Pre-op: Stop blood thinners, withhold movement disorder meds after midnight before surgery. NPO. Skin cleansing. Cognitive assessment.
- Post-op: Wound care (clean/dry, remove dressings day 3, gentle showering). Pain management (taper opioids). Activity restrictions (no heavy lifting, strenuous activity, driving for 2 weeks). Patient education: carry ID card, inform airport security, avoid large magnetic fields/heat therapy/electrocautery. DBS activated 3-4 weeks post-op.
Focused Ultrasound (FUS)
- Description: Non-invasive. Focused ultrasound beams create precise thermal lesions in brain targets (thalamus for tremor, globus pallidus for dyskinesia/rigidity) to disrupt abnormal circuits. No incision or implants.
- Indications: Tremor-dominated PD, Parkinson's dyskinesia, mobility, rigidity, slow initiation of movement. Currently unilateral, bilateral studies ongoing.
- Benefits: Non-invasive, avoids implant risks. Single procedure, no battery/wire maintenance. Potential for future drug delivery by opening blood-brain barrier.
- Risks/Complications: Sensory disturbances (numbness/tingling, temporary or permanent in 10-15%). Gait disturbance/imbalance (common temporarily, permanent in up to 10%). Minor: headache, pain, dizziness during procedure. Very low risk of stroke, infection, seizures.
- Nursing Care: Pre-procedure preparation. Monitor comfort/vitals during. Post-procedure: monitor side effects, educate on temporary symptoms, safety precautions for unsteadiness.
Nursing Care Plan
Holistic, patient-centered care with interprofessional collaboration. Goals: optimize motor function, enhance quality of life, maintain independence, promote stability, empower patients/caregivers.
Mobility
- Assessment: Motor function (tremors, gait, balance), ADL independence, fine motor skills, weakness, fatigue, stiffness.
- Interventions: PT referral. Assistive devices. Teach movement techniques (rocking to initiate, large steps, arm swing, lifting feet, visual cues for freezing, holding objects for tremor, warm baths for rigidity). Proper posture (firm mattress, prone positioning). Energy conservation. Avoid rushing.
Safety
- Fall Prevention: Remove hazards (rugs, clutter). Home modifications (grab bars, elevated toilets, chair lifts). Low-heeled shoes. Monitor gait/balance, especially during "off" periods.
- Medication Safety: Educate on dosage, route, action, side effects. Monitor for side effects (impaired balance, dizziness, sleepiness). Educate on drug-drug/drug-food interactions. Stress never stopping meds abruptly.
Nutrition
- Assessment: Swallowing function (dysphagia, aspiration risk), weight changes, constipation.
- Interventions: Dietitian collaboration (thickened liquids, pureed foods). Small, frequent, nutrient-dense meals. Increase fluids/fiber for constipation. Limit Vitamin B6 foods (can block levodopa).
Communication
- Assessment: Speech patterns (slurred, soft, monotone), ability to express.
- Interventions: Speech therapy referral. Encourage deep breaths, diaphragmatic speech. Suggest communication aids (amplifiers, boards). Allow ample response time.
Elimination
- Assessment: Constipation, urinary retention.
- Interventions: Increase fiber/fluids, encourage mobility for constipation. Monitor for urinary retention, discuss management.
Psychosocial Well-being
- Assessment: Emotional well-being (depression, anxiety, mood swings), cognitive function (memory, attention), caregiver strain.
- Interventions: Mental health professional referral. Support groups for patients/families. Patient/caregiver education on disease management, coping. Promote independence.
Patient And Family Education And Support
Empowering patients and families is crucial for active participation and coping.
Medication Adherence
- Importance of Schedule: Strict adherence for consistent symptom control.
- Reporting Side Effects: Promptly report new/bothersome symptoms.
- Never Stop Abruptly: Risk of severe complications.
- Interactions: Educate on food/drug interactions (protein, tyramine, B6, other meds, OTCs, supplements). Use single pharmacy.
Lifestyle Modifications
- Exercise: Only intervention potentially slowing progression. Regular cardio, resistance, flexibility, balance training.
- Diet and Nutrition: Manage constipation (fiber/fluids), optimize medication absorption (avoid high-protein with levodopa). Small, frequent meals.
- Sleep Hygiene: Promote good practices for sleep dysfunction.
Coping Strategies
- Mental Health Support: Encourage professional help for depression, anxiety.
- Support Groups: Provide emotional support, shared experiences, coping strategies.
- Adaptive Strategies: Guidance on adapting daily living as disease evolves.
Summary
- Parkinson's disease is a complex, progressive neurodegenerative disorder.
- It is defined by both motor symptoms (e.g., tremor, rigidity, bradykinesia) and non-motor symptoms (e.g., depression, sleep disturbances, autonomic dysfunction).
- The disease stems from dopaminergic neuron loss in the substantia nigra and alpha-synuclein protein aggregation.
- Diagnosis is clinical, often supported by neuroimaging and a positive response to levodopa therapy.
- Pharmacological treatments (e.g., levodopa, dopamine agonists) and non-pharmacological therapies (e.g., physical and occupational therapy) are essential for symptom control.
- Surgical options, such as deep brain stimulation, may be considered in advanced cases
