
Acquired Cardiovascular Disorders: Congestive Heart Failure
Lessons
- Objectives
- Introduction
- Epidemiology, Etiology, Risk Factors, And Pathophysiology
- Practice Excercise 1
- Classification
- Clinical Manifestations
- Diagnostic Evaluation
- Practice Excercise 2
- Therapeutic Management
- Nursing Care Plan
- Complications
- Prognosis
- Practice Excercise 3
- Summary
- Comprehensive Questions
Notes Highlighting is available once you sign in. Login Here.
Objectives
- Classify the underlying structural and acquired causes of congestive heart failure (CHF) within the pediatric population.
- Describe the compensatory mechanisms activated by the pediatric cardiovascular system in response to myocardial dysfunction.
- Identify the specific clinical manifestations that differentiate right-sided heart failure (systemic venous congestion) from left-sided heart failure (pulmonary congestion).
- Explain the pathophysiology of systemic and pulmonary fluid accumulation in infants and children.
- Interpret diagnostic evaluation findings, including chest X-rays, electrocardiograms, and echocardiograms, for a pediatric patient with heart failure.
- Outline the comprehensive therapeutic management options, prioritizing pharmacological interventions and nutritional strategies.
- Develop a highly structured nursing care plan and prioritize nursing interventions for an infant or child experiencing acute or chronic heart failure.
- Recognize potential life-threatening complications of pediatric CHF, including digitalis toxicity and metabolic exhaustion.
Introduction
- Congenital heart defects (CHDs) and acquired myocardial injuries characterized by systemic or pulmonary over-circulation represent the primary drivers of congestive heart failure (CHF) in the pediatric population.
- Unlike adult heart failure, which typically manifests as a chronic, secondary consequence of ischemic coronary artery disease or long-standing systemic hypertension, pediatric heart failure represents an acute or subacute structural or functional inability of the myocardium to meet the systemic metabolic and oxygen demands of a rapidly growing body.
- The pathophysiology of this disorder centers on a critical reduction in effective stroke volume and subsequent cardiac output. This physiological deficit triggers an immediate, multi-system neurohormonal cascade involving the sympathetic nervous system and the renin-angiotensin-aldosterone axis.
- Although these compensatory loops aim to preserve core perfusion pressures, their chronic activation imposes a severe dual burden: progressive fluid retention leads to systemic and pulmonary vascular volume overload, while persistent vasoconstriction increases myocardial workload, exhausting the limited physiological reserves of the immature pediatric ventricle.
- From a nursing perspective, recognizing pediatric heart failure demands a high index of clinical suspicion. Infants rarely present with obvious peripheral dependent edema or clear jugular venous distension; instead, they exhibit subtle, progressive signs of respiratory distress and systemic fatigue.
- A hallmark clinical sign is profound feeding intolerance. Because the metabolic cost of sucking and swallowing exceeds their compromised cardiorespiratory reserves, these infants become visibly diaphoretic, tachypneic, and exhausted during normal feeding cycles.
- This persistent mismatch between elevated energy expenditure and reduced caloric intake manifests as severe failure to thrive.
- Nurses must remain vigilant for these nuanced clinical transitions, formulating precise nursing diagnoses and implementing aggressive pharmacological, fluid, and nutritional interventions to optimize outcomes and support families through complex care trajectories.
Epidemiology, Etiology, Risk Factors, And Pathophysiology
Epidemiology & Etiology
Pediatric congestive heart failure is not a primary disease entity but rather a clinical syndrome resulting from an underlying structural or functional cardiac abnormality.
- Infants (Under 1 year): The vast majority of cases (greater than 80%) are caused by structural congenital heart defects (CHDs). These are predominantly left-to-right shunting defects (e.g., large VSD, PDA, AVSD) or obstructive lesions (e.g., Coarctation of the aorta, Hypoplastic left heart syndrome).
- Children and Adolescents: Acquired cardiovascular conditions dominate this demographic. These include myocarditis (often viral, such as Coxsackievirus B or Adenovirus), dilated or hypertrophic cardiomyopathies, rheumatic heart disease (RHD) following an untreated Group A beta-hemolytic Streptococcal pharyngeal infection, or chemotherapy-induced cardiotoxicity (e.g., doxorubicin).
Risk Factors
- Prenatal Factors: Maternal diabetes, maternal lupus, intrauterine viral exposure (rubella, CMV), and advanced maternal age.
- Genetic and Chromosomal Syndromes: Down syndrome (Trisomy 21), Turner syndrome, Williams syndrome, and DiGeorge syndrome (22q11.2 deletion).
- Acquired Conditions: Severe, uncorrected chronic anemia, chronic renal failure causing fluid overload, or acute bacterial endocarditis.
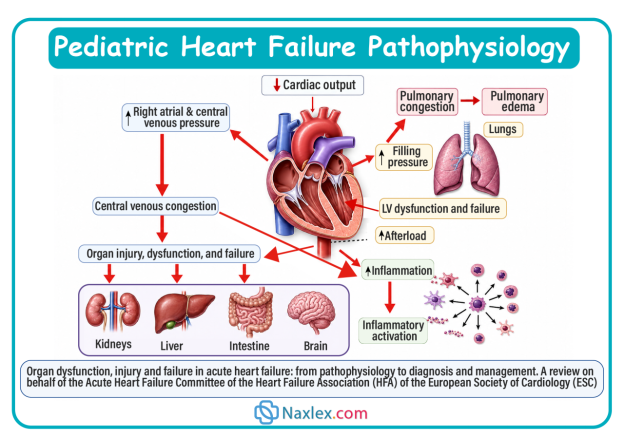
Pathophysiology & Compensatory Mechanisms
When cardiac output falls below the metabolic demands of the pediatric tissues, the body initiates three primary compensatory pathways to maintain homeostasis. Although helpful in the short term, their sustained activation damages the heart muscle.
- Sympathetic Nervous System (SNS) Stimulation:
- Decreased systemic perfusion stimulates baroreceptors, triggering the release of epinephrine and norepinephrine.
- This results in tachycardia (to boost cardiac output) and increased systemic vascular resistance (vasoconstriction), shifting blood toward vital organs but raising the workload (afterload) the heart must pump against.
- Renin-Angiotensin-Aldosterone System (RAAS) Activation:
- Reduced renal perfusion prompts the kidneys to secrete renin, converting angiotensinogen to angiotensin I, which is converted to angiotensin II by ACE.
- Angiotensin II causes potent systemic vasoconstriction and stimulates the adrenal cortex to release aldosterone, causing significant sodium and water retention. This elevates blood volume (preload), leading to systemic and pulmonary edema.
- Myocardial Structural Remodeling:
- The heart muscle fibers stretch to accommodate the increased blood volume (ventricular dilation) to increase contractility via the Frank-Starling law. Over time, chronic wall stress leads to ventricular hypertrophy (thickening of the muscle walls), which increases myocardial oxygen demand and decreases ventricular compliance.
Image Title: Pediatric Heart Failure Pathophysiology
Classification
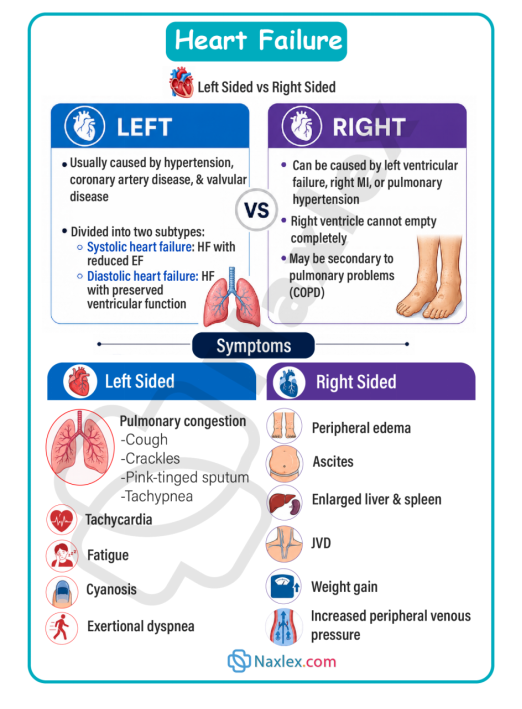
Pediatric heart failure can be classified based on the anatomical side of the heart that is primarily dysfunctional, or by the clinical presentation of systemic versus pulmonary symptoms.
Right-Sided Heart Failure
- Definition: The right ventricle is unable to pump blood effectively into the pulmonary artery.
- Mechanism: Backpressure develops in the right atrium, leading to venous congestion in the systemic circulation.
- Primary Causes: Pulmonic stenosis, uncorrected left-to-right shunts (causing secondary right ventricular strain), or pulmonary hypertension.
Left-Sided Heart Failure
- Definition: The left ventricle is unable to pump blood into the systemic circulation.
- Mechanism: Pressure increases in the left atrium, backing blood up into the pulmonary veins and capillaries.
- Primary Causes: Large VSD, PDA, Coarctation of the Aorta, Aortic Stenosis, or acute myocarditis.
High-Output Heart Failure
- Definition: The heart muscle is structurally normal and pumping at or above capacity, but cannot satisfy the body's unusually high metabolic demands.
- Primary Causes: Severe chronic anemia, systemic arteriovenous fistulas, or severe hyperthyroidism.
Clinical Manifestations
Children with heart failure present with signs related to systemic venous congestion, pulmonary congestion, and low systemic cardiac output.
Right-Sided Heart Failure (Systemic Venous Congestion)
- Hepatomegaly: Tenderness and palpable liver edge more than 2 cm below the right costal margin (caused by portal venous pooling).
- Periorbital edema: Fluid accumulation in the loose tissues around the eyes, especially visible in the morning.
- Sudden weight gain: A reliable indicator of fluid retention in infants, preceding noticeable dependent edema.
- Peripheral edema: Seen in older children as pitting edema over the shins, ankles, or sacrum.
- Distended jugular veins: Evident in older pediatric patients; rare in infants due to short neck anatomy.
Left-Sided Heart Failure (Pulmonary Congestion)
- Tachypnea: Respiratory rates exceeding 60 breaths/minute in infants, driven by fluid-congested, stiff lungs.
- Dyspnea, orthopnea, and retractions: Increased work of breathing with intercostal, subcostal, and suprasternal retractions, nasal flaring, and expiratory grunting.
- Pulmonary crackles/wheezing: Auscultated over the lung bases due to fluid accumulation in alveolar and interstitial spaces.
- Persistent dry cough: Caused by bronchial mucosal edema or compression of the left main bronchus by an enlarged left atrium.
Cardiac Assessment Findings
A targeted physical assessment of the cardiovascular system reveals objective data regarding myocardial dysfunction and compensatory adaptations:
- Tachycardia: A persistent, resting heart rate elevated above normal developmental limits (e.g., sleeping infant heart rate greater than 160 bpm; child heart rate greater than 100 bpm). This is the earliest sign of heart failure.
- Abnormal Heart Sounds (Gallop Rhythm): Auscultation often reveals an S3 or S4 gallop rhythm, which represents ventricular filling delays and altered wall compliance in a volume-overloaded or stiff ventricle.
- Pathological Murmurs: Distinct structural murmurs help pinpoint the underlying cause (e.g., a loud, harsh holosystolic murmur at the lower left sternal border for a VSD, or a continuous machinery-like murmur beneath the left clavicle for a PDA).
- Precordial Activity: An active precordium, parasternal lifts, or displaced Point of Maximal Impulse (PMI) inferiorly or laterally due to ventricular dilation and hypertrophy.
- Diminished Peripheral Pulses: Systemic vasoconstriction creates weak, thready peripheral pulses (brachial, radial, pedal) compared to strong, bounding central pulses (femoral, carotid).
- Altered Tissue Perfusion: Cool, pale, or mottled extremities with a delayed capillary refill time greater than 3 seconds.
Impaired Cardiac Output & Increased Metabolic Demand
- Feeding intolerance: The infant becomes diaphoretic (sweaty), particularly on the forehead, and grows exhausted after taking only a small volume of formula or breast milk.
- Failure to thrive (FTT): Poor weight gain and linear growth retardation because the child burns excessive calories simply trying to breathe.
- Tachycardia: Resting heart rate persistently elevated above normal limits for age (e.g., greater than 160 bpm in sleeping infants) due to sympathetic drive.
- Weak peripheral pulses and delayed capillary refill: Reduced perfusion to extremities leads to pale, mottled, or cool skin and a capillary refill time greater than 2 to 3 seconds.
Chronic Signs of Hypoxemia
When heart failure is caused by cyanotic heart disease or advanced, uncorrected left-to-right shunting that has transitioned into pulmonary hypertension (Eisenmenger syndrome), chronic cellular hypoxia triggers distinct physical adaptations:
- Digital Clubbing: Proliferation of vascular connective tissue beneath the nail beds of the fingers and toes, causing the profile angle between the nail and the nail base to exceed 180 degrees. This results from chronic capillary hypoxia and the localized release of growth factors.
- Polycythemia: In response to chronic hypoxia, the kidneys increase erythropoietin production, stimulating bone marrow to produce excess red blood cells. While this raises oxygen-carrying capacity, it increases blood viscosity and escalates the risk of thromboembolic events (e.g., stroke).
- Squatting Posture (Knee-Chest Positioning): Seen in walking children during episodes of exertion or hypoxemia. Squatting mechanically increases systemic vascular resistance, reducing right-to-left shunting and forcing more blood through the lungs to improve oxygenation.
- Chronic Cyanosis: A persistent bluish discoloration of the mucous membranes, tongue, and nail beds, indicating that unoxygenated hemoglobin levels exceed 5g/dL.
Diagnostic Evaluation
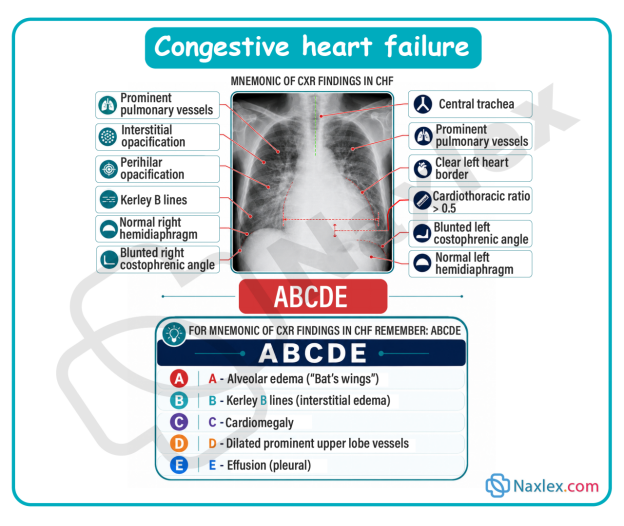
Chest X-Ray (CXR)
- Cardiomegaly: Reveals an enlarged heart silhouette (cardiothoracic ratio greater than 55% in infants or greater than 50% in older children).
- Pulmonary congestion: Shows prominent pulmonary vascular markings, interstitial edema, and pleural effusions.
Electrocardiogram (ECG)
- Chamber hypertrophy: Shows increased voltage waves indicating right, left, or biventricular hypertrophy.
- Arrhythmias: Identifies sinus tachycardia, atrial flutter, or premature ventricular contractions resulting from myocardial stretch.
-
Echocardiogram (Echo)
- Anatomical assessment: The primary tool used to diagnose underlying congenital heart defects or confirm cardiomyopathy.
- Functional measurement: Measures ejection fraction (EF) and fractional shortening (FS) to quantify left ventricular systolic function, and tracks structural wall thickness.
-
Laboratory Biomarkers
- Brain natriuretic peptide (BNP): Released by ventricular myocytes in response to high wall stretch and volume overload; used to differentiate cardiac from primary respiratory causes of distress.
- Serum Electrolytes: Evaluated frequently because renal hypoperfusion can alter sodium and potassium balance, which is further modified by diuretic therapies.
Therapeutic Management
The main objectives of therapeutic management are to reduce volume overload (preload), decrease systemic vascular resistance (afterload), and improve myocardial contractility.
Pediatric CHF Medication Guide
|
Medication Class |
Mechanism of Action (MOA) |
Examples |
Indications |
Precautions / Contraindications |
Parameters to Monitor |
Nursing Insights & Side Effects |
|
Cardiac Glycosides |
Inhibits the sodium-potassium ATPase pump, increasing intracellular calcium concentration to boost myocardial contractility (positive inotrope) while prolonging the AV node refractory period to slow the heart rate (negative chronotrope). |
Digoxin (Lanoxin) |
Increases force of myocardial contraction; increases cardiac output while slowing heart rate. |
Contraindicated in ventricular fibrillation or heart block. Hold if apical pulse is less than 90–110 bpm in infants or less than 70 bpm in older children. |
• Apical pulse (1 full minute) • Serum potassium levels • Serum digoxin levels (0.5-2.0 ng/mL) • Renal function (BUN/creatinine) |
Narrow therapeutic index. Toxicity signs include bradycardia, anorexia, and unexplained vomiting. Hypokalemia significantly increases the risk of digoxin toxicity. |
|
Loop Diuretics |
Inhibits the Na+/K+/2Cl- cotransporter in the thick ascending loop of Henle, blocking the reabsorption of sodium, chloride, and water, which drives rapid fluid excretion. |
Furosemide (Lasix) |
Decreases intravascular volume (preload) by inducing rapid diuresis; resolves pulmonary and systemic edema. |
Contraindicated in anuria. Use with extreme caution in pre-existing severe electrolyte depletion. |
• Daily weights at identical times • Strict intake/output (I/O) volumes • Serum electrolytes (especially K+, Cl-, Na+) • Blood pressure |
Causes hypokalemia, hypochloremia, and dehydration. Ototoxicity can occur with rapid intravenous push. Monitor for muscle weakness or cramping due to low potassium. |
|
Potassium-Sparing Diuretics |
Competitively antagonizes aldosterone receptors in the distal convoluted tubule and collecting duct, blocking sodium-water reabsorption while conserving potassium ions. |
Spironolactone (Aldactone) |
Weak diuretic; used as an adjunct to loop diuretics to prevent potassium wasting while managing fluid retention. |
Contraindicated in acute renal failure, anuria, or pre-existing hyperkalemia. |
• Serum potassium and sodium • Renal function markers (BUN/creatinine) • Blood pressure |
Risk of hyperkalemia, especially if given with ACE inhibitors. Avoid potassium supplements or excessive dietary potassium intake. Assure adequate urine output before giving. |
|
ACE Inhibitors |
Blocks the Angiotensin-Converting Enzyme, preventing the conversion of Angiotensin I to the potent vasoconstrictor Angiotensin II. This promotes systemic vasodilation, reduces aldosterone secretion, and decreases afterload. |
Captopril, Enalapril |
Reduces afterload by promoting systemic vasodilation, making it easier for the weak ventricle to pump blood forward. |
Contraindicated in cases of angioedema or pregnancy. Caution with concurrent potassium-retaining medications. |
• Blood pressure (before and after) • Serum potassium • Renal function (creatinine) • White blood cell count |
Monitor blood pressure closely for profound hypotension, especially after the first dose. Watch for a persistent, dry ACE cough and hyperkalemia. |
Nutritional and Supportive Care
- High-calorie density feeding: Standard formula or breast milk (20 kcal/oz) is often concentrated to 24 to 30 kcal/oz using commercial fortifiers or glucose polymers. This delivers essential calories in a smaller fluid volume, preventing volume overload.
- Feeding schedule optimization: Limit active nipple feedings (breast or bottle) to a maximum of 20 to 30 minutes to minimize energy expenditure. Administer the remaining volume or entire feed via a gavage/nasogastric (NG) tube if the infant exhibits respiratory distress or fatigue.
- Oxygen administration: Administer supplemental humidified oxygen with caution.
Critical Safety Note: In infants with large left-to-right shunts (like VSD or PDA), oxygen acts as a potent pulmonary vasodilator. Giving too much oxygen can reduce pulmonary vascular resistance further, worsening the left-to-right shunt and flooding the lungs.
Nursing Insight: Administer pediatric CHF medications at the same times daily, ideally one hour before or two hours after feeds, using a calibrated oral syringe. Do not mix the medications directly into formula or breast milk bottles, as the infant may not finish the entire volume, resulting in an incomplete dose. Never readminister a dose if the child vomits. If a dose is missed by less than 4 hours, give it immediately; if over 4 hours, skip it. Never double doses. Contact the provider if two consecutive doses are missed.
Nursing Care Plan
Priority Nursing Diagnoses (NANDA-I Framework)
- Decreased Cardiac Output related to structural myocardial defects or altered myocardial contractility as evidenced by tachycardia, weak peripheral pulses, and delayed capillary refill.
- Excess Fluid Volume related to activation of the renin-angiotensin-aldosterone axis and compromised renal perfusion as evidenced by hepatomegaly, periorbital edema, and rapid weight gain.
- Ineffective Breathing Pattern related to pulmonary venous congestion and fluid accumulation within the alveoli as evidenced by tachypnea, grunting, nasal flaring, and intercostal retractions.
- Imbalanced Nutrition: Less Than Body Requirements related to high metabolic work of breathing and feeding intolerance as evidenced by inability to finish feeds, diaphoresis during feeding, and weight loss or failure to thrive.
Nursing Interventions & Rationales
The Strategy of Clustering Care
The organizing principle of pediatric heart failure nursing care is clustering care. This involves grouping multiple assessments, medication administrations, and nursing tasks into a single, coordinated block of time, followed by long, uninterrupted rest periods.
- Assess Patient State and Plan Layout (Pre-intervention): Review the schedule. Coordinate with laboratory, radiology, and therapy teams so all diagnostic samplings align with the planned nursing block. Never wake an infant just to check a routine parameter unless clinically unstable.
- Execute Clustered Nursing Tasks (Maximum 15–20 minutes): Gently perform essential interventions in a single session: check vital signs, auscultate heart and lung sounds, weigh the infant (if indicated), change diapers, and administer cardiac medications. Keep environmental stimuli, such as bright lights and loud noises, to a absolute minimum.
- Deliver High-Density Nutrition: Administer fortified, high-calorie nutrition. If the infant is bottle-feeding, stop at the 20-to-30-minute mark. Administer any remaining volume via the nasogastric tube while the infant rests to prevent metabolic exhaustion.
- Position for Optimal Ventilation: Place the infant in an elevated semi-Fowler or high-Fowler position (using an infant seat or elevating the head of the bed to a 30-to-45-degree angle). This lowers the diaphragm, maximizing chest expansion and decreasing venous return to ease the workload on the heart.
- Enforce Extended, Uninterrupted Rest (2 to 3 hours): Dim the lights, cluster family support at the bedside, and leave the infant completely undisturbed. This reduces the sympathetic drive, lowering the heart rate and blood pressure, which conserves energy and limits oxygen demand.
Complications
Digitalis (Digoxin) Toxicity
Because pediatric patients have immature renal clearance systems, they are at high risk for Digoxin toxicity.
- Clinical presentation: Bradycardia, poor feeding, nausea, and frequent vomiting (often mistaken for spitting up).
- Antidote: Digoxin Immune Fab (Digibind) is administered for severe, life-threatening arrhythmias or toxic serum levels.
Metabolic Exhaustion and Failure to Thrive
If caloric density cannot compensate for the high energy expenditure of breathing, the child's body breaks down muscle and fat stores. This results in severe linear growth failure, delayed cognitive development, and a weakened immune system.
Cardiopulmonary Collapse
Acute decompensation can occur when compensatory mechanisms fail. This leads to profound cardiogenic shock, severe pulmonary edema, severe metabolic acidosis, and multi-organ failure.
Prognosis
The long-term outlook for a child with heart failure depends heavily on whether the primary cause can be reversed or surgically corrected.
- Surgically correctable defects: Children with left-to-right shunts (VSD, ASD, PDA) show rapid resolution of heart failure symptoms and excellent catch-up growth once the defect is closed.
- Chronic cardiomyopathies: Structural heart muscle diseases have a more guarded prognosis. If medical management fails to halt ventricular remodeling, these patients may require long-term mechanical circulatory support (Ventricular Assist Devices) or a cardiac transplant.
Summary
- Congestive heart failure (CHF) in pediatric patients is a complex clinical syndrome characterized by the heart's inability to pump an adequate supply of oxygenated blood to meet the metabolic demands of the body.
- In infants, the condition is almost exclusively driven by structural congenital heart defects that cause a left-to-right shunt (such as ventricular septal defects or patent ductus arteriosus). These defects flood the pulmonary system with excess fluid volume.
- In older children, heart failure is more often an acquired condition resulting from viral myocarditis, cardiomyopathies, or rheumatic heart disease.
- When cardiac output drops, the pediatric body activates neurohormonal pathways, specifically the sympathetic nervous system and the renin-angiotensin-aldosterone system.
- Although these systems maintain core blood pressure via tachycardia, vasoconstriction, and fluid retention, their chronic activation overloads the heart chambers and causes systemic and pulmonary edema.
- The clinical presentation in children varies by age, with infants showing distinct signs of distress.
- Left-sided heart failure causes pulmonary congestion, which manifests as tachypnea, grunting, intercostal retractions, and rales. Right-sided heart failure causes systemic venous congestion, leading to hepatomegaly, periorbital edema, and sudden fluid weight gain.
- A key clinical feature of pediatric heart failure is feeding intolerance, where infants become diaphoretic and exhausted during feeds, resulting in failure to thrive because their caloric needs outpace their intake.
- Diagnostic evaluation relies on chest X-rays to assess for cardiomegaly, ECGs to screen for hypertrophy or arrhythmias, and echocardiograms to evaluate ventricular function and visualize structural defects.
- Therapeutic management focuses on reducing fluid volume with loop diuretics (Furosemide), decreasing afterload with ACE inhibitors, and improving contractility with cardiac glycosides (Digoxin).
- Nutritional adjustments are critical; nurses must provide high-calorie, concentrated formulas and limit active feeding times to under 30 minutes, using nasogastric gavage for any remaining volume to prevent metabolic exhaustion.
- The core nursing responsibilities include monitoring fluid balance through daily weights and precise intake/output measurements, watching for signs of Digoxin toxicity (such as bradycardia or vomiting), and supporting the child's respiratory effort.
- The long-term prognosis is excellent for children with correctable structural defects, but remains guarded for those with progressive cardiomyopathies who may ultimately require cardiac transplantation.
