
Growth And Development In Toddlers
Lessons
Notes Highlighting is available once you sign in. Login Here.
Objectives
- Articulate the key developmental milestones across biologic, cognitive, moral, spiritual, body image, gender identity, and social domains in toddlers (ages 1-3 years).
- Identify nursing interventions that promote optimum growth and development in toddlers, considering their unique needs and vulnerabilities.
- Discuss common concerns related to normal toddler growth and development.
- Analyze the impact of temperament on toddler behavior and development, and apply this understanding to individualized nursing care.
- Develop evidence-based strategies for promoting optimum health during toddlerhood, encompassing nutrition, sleep, activity, dental health, and injury prevention.
- Integrate knowledge of complementary and alternative medicine (CAM) and vegetarian diets into the nutritional counseling of parents of toddlers, recognizing potential benefits and risks.
- Educate parents and caregivers on age-appropriate safety measures to prevent common injuries in toddlers.
- Apply the nursing process to assess, plan, implement, and evaluate care for toddlers and their families, fostering healthy growth and development.
Introduction
- The toddler years, spanning from ages one to three, represent a critical transition from the total dependency of infancy to the burgeoning autonomy of early childhood.
- For the pediatric nurse, this stage is characterized by the "quest for independence," often manifested through the classic toddler traits of negativism and ritualism.
- Biologically, physical growth slows compared to infancy, a phenomenon known as "physiologic anorexia", as the child’s focus shifts from caloric intake to the mastery of gross and fine motor skills.
- This period is not merely a physical journey but a profound psychological one, as the toddler begins to navigate the tension between their desire for self-assertion and their inherent need for parental security.
- Developmentally, the toddler is operating within Piaget’s sensorimotor and early preoperational phases, where they begin to use symbols and language to represent their world. This cognitive shift is mirrored by Erikson’s stage of Autonomy vs. Shame and Doubt, where the successful mastery of tasks like feeding themselves or dressing leads to a sense of self-control.
- Nurses must also recognize the emergence of the toddler’s moral and spiritual identity; at the preconventional level, "right" and "wrong" are defined simply by the physical consequences of an action.
- As they explore their environment, toddlers also begin to form a rudimentary body image and gender identity, often influenced by the reactions and reinforcements of their primary caregivers.
- Understanding the toddler's temperament is vital for nursing practice, as it dictates how the child responds to the stressors of the clinical environment.
- A toddler’s social development is marked by "parallel play," where they play alongside others but not necessarily with them.
- By understanding these foundational principles, nurses can provide anticipatory guidance that validates the toddler’s need for autonomy while ensuring they remain within a safe, structured, and supportive framework.
Promoting Optimum Growth And Development
Promoting optimum growth and development in toddlers requires a holistic approach, considering all aspects of their physical, cognitive, social, and emotional well-being. Nurses act as educators, advocates, and care providers, guiding parents through this dynamic stage.
3.1. Biologic Development
Biologic development in toddlers is marked by significant physical growth and maturation of body systems. While growth slows compared to infancy, it remains rapid.
- Weight: On average, toddlers gain approximately 4 to 6 pounds (1.8 to 2.7 kg) per year. By 2.5 years, their birth weight has quadrupled.
- Height: Toddlers grow about 3 inches (7.5 cm) per year.
- Head Circumference: Head growth continues, but at a slower pace than in infancy, reflecting continued brain development. By 2 years, head circumference is typically 90% of adult size.
- Fontanels: The anterior fontanel typically closes between 12 and 18 months of age.
- Body Proportions: The toddler's body proportions change, with the trunk and extremities growing faster, giving them a more elongated appearance than infants.
Nursing Insight: Deviations from expected growth curves such as weight, height, and head circumference can signal underlying health issues requiring further investigation.
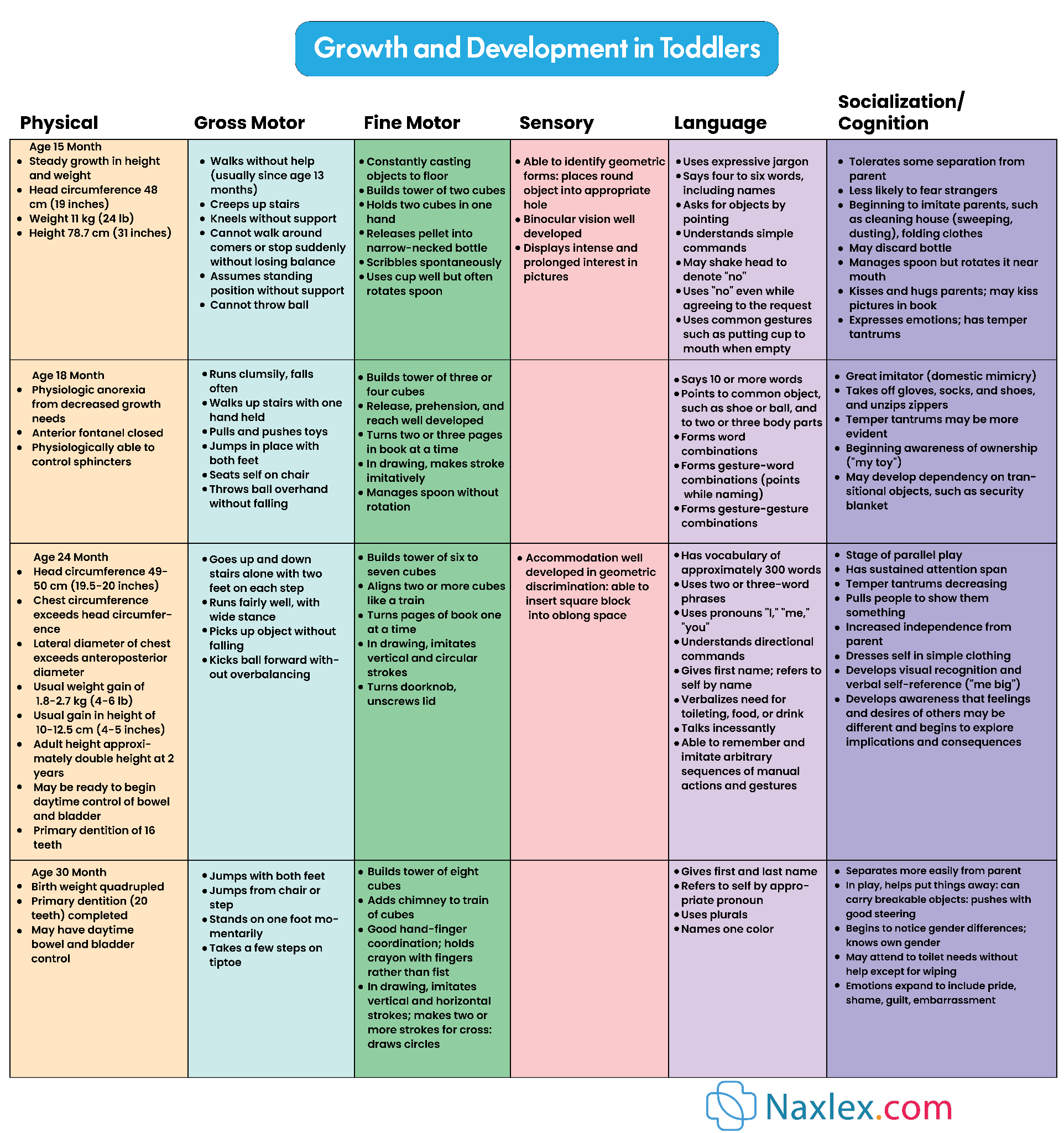
- Gross Motor Skills:
- 12-15 months: Walks independently, creeps up stairs, stands without support, stoops and recovers.

-
- 18 months: Runs stiffly, throws a ball overhand (without much accuracy), jumps in place with both feet, pulls/pushes toys.
- 24 months: Walks up and down stairs holding on, kicks a ball forward, stands on tiptoes, builds a tower of 6-7 blocks.
- 30 months: Jumps with both feet, stands on one foot momentarily, takes a few steps on tiptoes.
- 36 months: Rides a tricycle, alternates feet going up stairs, jumps over objects.
- Fine Motor Skills:
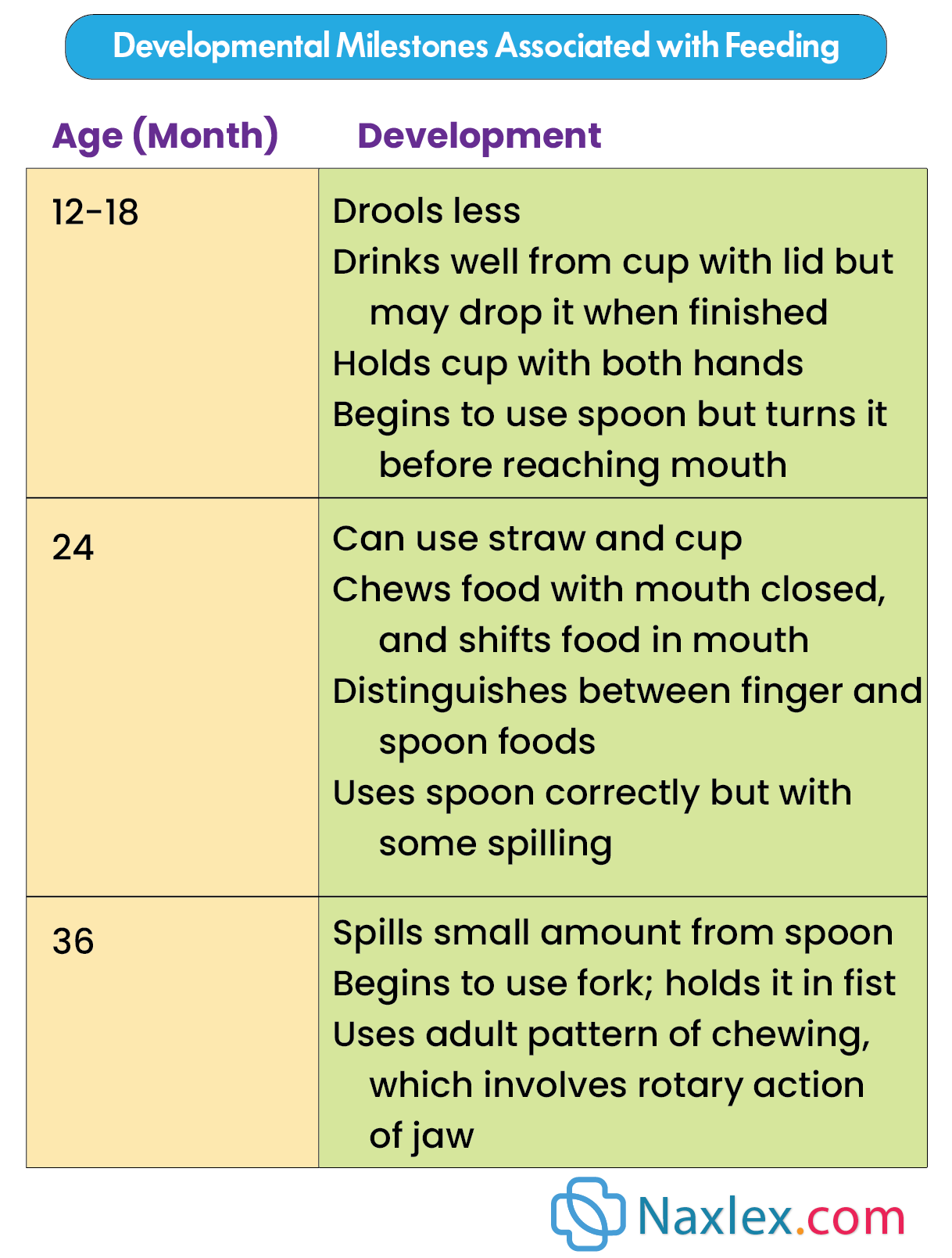
- 12-15 months: Uses a cup well, builds a tower of 2 blocks, scribbles spontaneously.
- 18 months: Manages a spoon without rotating, turns pages in a book (two or three at a time), builds a tower of 3-4 blocks, imitates drawing a vertical line.
- 24 months: Builds a tower of 6-7 blocks, imitates drawing a horizontal line, completes simple puzzles (3-4 pieces), unbuttons large buttons.
- 30 months: Draws circles, copies a cross, builds a tower of 8 blocks.
- 36 months: Copies a circle, draws a person with 2-3 parts, uses blunt scissors.
- Physiological Systems:
- Respirations: Slows to 25-30 breaths per minute. Airways are still relatively small, making toddlers susceptible to respiratory infections.
- Heart Rate: Slows to 80-110 beats per minute.
- Blood Pressure: Increases to approximately 90/50 mmHg.
- Thermoregulation: Improves but toddlers are still vulnerable to extreme temperatures.
- Immune System: Continues to mature, but toddlers still experience frequent infections, especially if in group childcare settings. Maternal antibodies are decreasing.
- Gastrointestinal System: Digestive processes mature, allowing for a wider variety of foods. Bowel control develops later.
- Renal System: Kidneys mature, and bladder capacity increases, contributing to readiness for toilet training.
Nursing Implications for Biologic Development:
- Monitor growth parameters (weight, height, head circumference) regularly and plot on growth charts.
- Provide anticipatory guidance on age-appropriate gross and fine motor skill development.
- Encourage opportunities for active play and exploration to enhance motor development.
- Educate parents on normal physiological changes and signs of illness.
- Advise on appropriate sleep patterns and rest.
- Emphasize the importance of a balanced diet for optimal physical growth.
3.2. Cognitive Development (Piaget: Sensorimotor and Preoperational Phases)
Toddlers are in the latter part of Piaget's sensorimotor stage and are transitioning into the preoperational stage.
- Sensorimotor Stage (12-24 months):
- Tertiary Circular Reactions (12-18 months): Toddlers actively experiment with objects, trying out new behaviors to see what happens (e.g., dropping a spoon repeatedly). They use trial-and-error to solve problems.
- Invention of New Means Through Mental Combinations (18-24 months): Toddlers begin to think before they act. They can solve problems in their minds and understand cause-and-effect relationships more abstractly. Object permanence is fully developed. They engage in domestic mimicry (imitating household activities).
- Preoperational Stage (2-7 years):
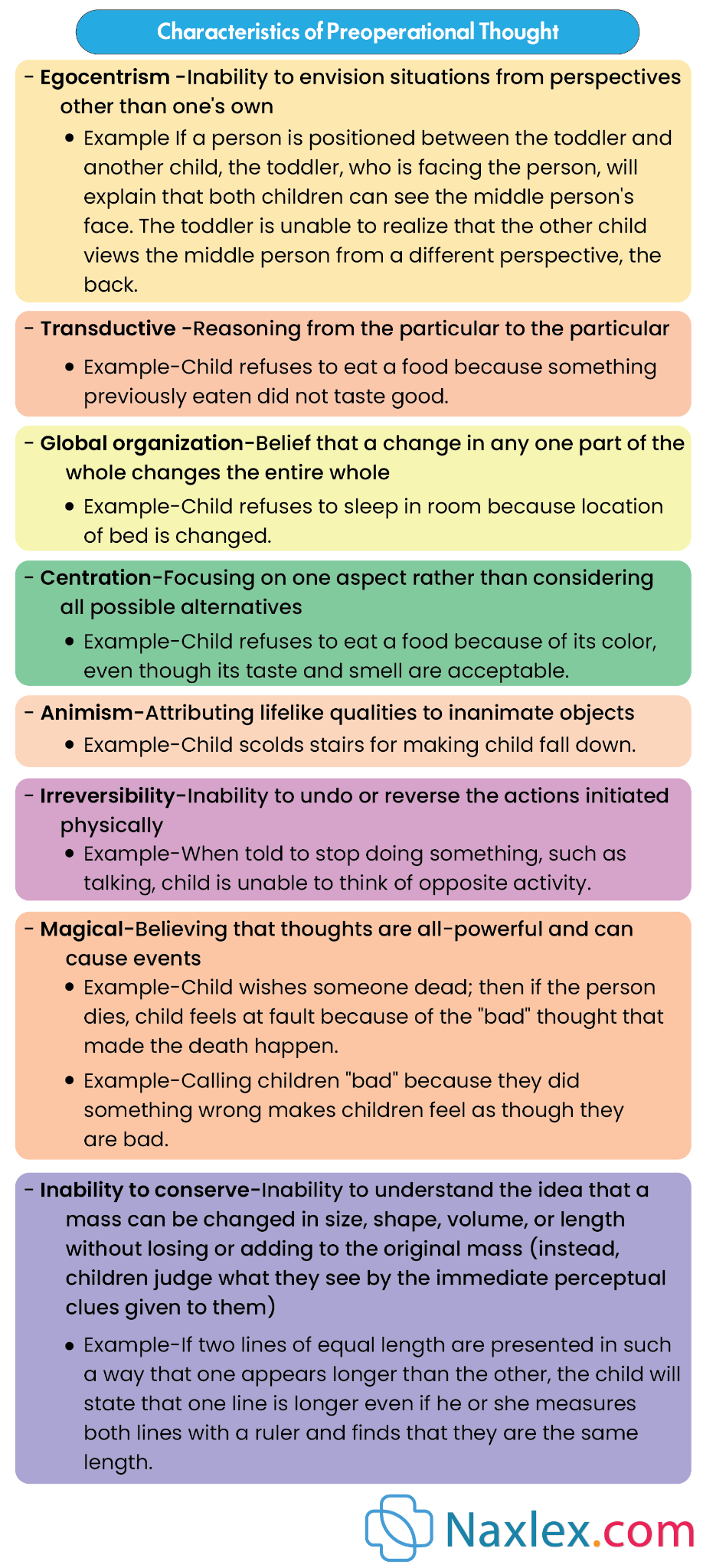
- Preconceptual Phase (2-4 years): This phase is marked by the beginning of symbolic thought.
- Egocentrism: Toddlers are unable to see situations from another person's perspective. They believe everyone sees the world as they do.
- Transductive Reasoning: Toddlers connect particular experiences, whether or not there is a logical casual relationship (e.g., "The sun sets because I go to bed").
- Animism: Attributing lifelike qualities to inanimate objects (e.g., "The doll is sad").
- Magical Thinking: Believing that thoughts or actions can cause events to happen (e.g., "If I wish for it, it will happen").
- Global Organization: If one aspect of a situation changes, the whole situation changes (e.g., new clothes mean a new identity).
- Centration: Focusing on one aspect of a situation and neglecting other important features.
- Irreversibility: Inability to mentally reverse a sequence of events or operations.
- Preconceptual Phase (2-4 years): This phase is marked by the beginning of symbolic thought.
-
- Language Development:
- 12-15 months: Uses 4-6 words, imitates animal sounds, babbles with inflection.
- 18 months: Uses 10-20 words, uses two-word phrases ("want cookie"), points to familiar objects.
- 24 months: Uses 300 words, uses 2-3 word sentences, asks "what?" and "where?" questions, names familiar objects and body parts.
- 36 months: Uses 900-1000 words, uses 3-4 word sentences, uses pronouns (I, you, me), understands most of what is said, can give first name and age.
- Language Development:
- Concept of Time and Space: Still limited to "now" and "here."
- Problem Solving: Moves from trial and error to more thoughtful approaches.
Nursing Implications for Cognitive Development:
- Provide opportunities for play that encourages exploration and problem-solving (e.g., stacking toys, simple puzzles).
- Engage in conversations with toddlers, encouraging language development through repetition, clear pronunciation, and expanding on their utterances.
- Read aloud to toddlers daily to foster language and cognitive skills.
- Acknowledge and respect their egocentric perspective, understanding it's a normal part of development.
- Use simple, concrete language when communicating with toddlers.
- Explain procedures in a way they can understand, using their level of cognitive development.
3.3. Moral Development - Preconventional or Premoral Level (Kohlberg)
According to Kohlberg, toddlers are in the preconventional or premoral level of moral development, specifically in Stage 1: Obedience and Punishment Orientation.
- Stage 1: Obedience and Punishment Orientation:
- Toddlers' decisions about right and wrong are based primarily on avoiding punishment and obtaining rewards.
- They do not yet understand the underlying reasons for rules; they simply obey to avoid negative consequences.
- Behaviors are judged as "good" or "bad" based on their immediate outcomes.
- Punishment is seen as a sign of badness, and obedience is a way to avoid it.
Nursing Insight: Behavior is motivated by reward/punishment. Discipline must be consistent, immediate, and focused on the action, not the child. Avoid shaming.
Nursing Implications for Moral Development:
- Set clear, consistent limits and consequences for behavior.
- Use positive reinforcement for desired behaviors.
- Explain rules in simple terms, focusing on the immediate impact (e.g., "Don't touch the stove, it's hot and will hurt you").
- Avoid lengthy explanations or abstract reasoning, as toddlers cannot grasp these.
- Focus on teaching simple concepts of right and wrong through consistent discipline and modeling.
3.4. Spiritual Development
Spiritual development in toddlers is largely influenced by their environment and the beliefs and practices of their primary caregivers.
- Learning through Imitation: Toddlers absorb spiritual concepts and rituals through observing and imitating their parents and family members.
- Concrete Understanding: Their understanding of spiritual concepts is very concrete and literal. Abstract ideas about God or spirituality are beyond their comprehension.
- Rituals and Routines: They may enjoy participating in religious rituals and routines, not necessarily understanding their meaning, but finding comfort and familiarity in them.
- Sense of Wonder: They have a natural sense of wonder and curiosity about the world around them, which can be a foundation for spiritual exploration later.
Nursing Insight: Spiritual understanding is concrete and imitative. Respect family's spiritual practices and accommodate rituals if they provide comfort. Avoid abstract spiritual discussions.
Nursing Implications for Spiritual Development:
- Respect the family's religious and spiritual beliefs and practices.
- Inquire about and accommodate family rituals that provide comfort (e.g., bedtime prayers).
- Recognize that spiritual development at this age is primarily observational and imitative.
- Avoid imposing religious views on families.
3.5. Development of Body Image
The development of body image in toddlers is a crucial aspect of their self-concept.
- Recognizing Self: Toddlers begin to recognize themselves as distinct from others, initially through self-recognition in mirrors and photographs.
- Labeling Body Parts: They learn to identify and name various body parts.
- Body Integrity: They have a developing, but still fragile, sense of body integrity. Minor injuries or procedures can be perceived as significant threats to their wholeness. They may believe their "insides" will fall out if they have a small cut.
- Gender Differences: They begin to recognize gender differences in body parts.
- Dress-Up and Imitation: They enjoy dressing up and imitating adult roles, which contributes to their understanding of body and self.
Nursing Implications for Development of Body Image:
- Use correct anatomical terms for body parts.
- Reassure toddlers about their body integrity during procedures or injuries.
- Allow them to explore their bodies (within appropriate boundaries) and answer their questions simply and directly.
- Minimize invasive procedures when possible, and prepare toddlers for them using age-appropriate language and visual aids.
- Encourage self-care activities like dressing and undressing to foster body awareness.
3.6. Development of Gender Identity
Gender identity, the inner sense of being male or female, begins to develop during toddlerhood.
- Awareness of Gender: Toddlers become aware of their own gender and that of others.
- Gender-Typed Play: They begin to engage in gender-typed play, often imitating the roles of same-sex adults.
- Labeling Gender: They can correctly label themselves and others as "boy" or "girl."
- Parental Influence: Parental attitudes and societal expectations heavily influence the development of gender identity.
Nursing Implications for Development of Gender Identity:
- Avoid gender stereotypes in play and language, allowing children to explore various interests.
- Support parents in fostering a positive self-image regardless of gender.
- Recognize that variations in gender expression are normal, and provide a supportive environment.
- Use inclusive language.
3.7. Social Development (Erikson: Autonomy vs. Shame and Doubt)
According to Erikson, toddlerhood is characterized by the psychosocial crisis of autonomy versus shame and doubt.
- Autonomy: Toddlers strive for independence and control over their own bodies and environment. They want to do things for themselves (e.g., feed themselves, dress themselves). This is expressed through their frequent use of "no!" and desire for choices.
- Shame and Doubt: If toddlers are consistently shamed, ridiculed, or overcontrolled when attempting to exert autonomy, they may develop feelings of shame and doubt about their abilities and sense of self-worth.
- Differentiation of Self from Others: Toddlers are increasingly aware of themselves as separate individuals.
- Social Interactions:
- Parallel Play: Toddlers typically engage in parallel play, playing alongside other children but not directly interacting with them. They may observe each other but are largely self-focused.
- Imitation: They love to imitate the actions of adults and older children.
- Brief Cooperative Play: Towards the end of toddlerhood, brief episodes of cooperative play may emerge.
- Separation Anxiety: While typically less intense than in infancy, separation anxiety can still occur, especially in unfamiliar situations.
- Stranger Anxiety: Also less pronounced but can still be present.
- Negativism: A characteristic behavior where toddlers frequently say "no" or refuse to comply, as a way to assert their developing autonomy.
- Ritualism: The need for sameness, routine, and predictability. This provides a sense of security and control in a rapidly changing world. Deviations from rituals can cause distress.
- Possessiveness: Toddlers often have a strong sense of ownership over their toys and possessions and may have difficulty sharing.
Nursing Implications for Social Development:
- Provide opportunities for toddlers to make simple choices (e.g., "Do you want to wear the red shirt or the blue shirt?").
- Encourage self-feeding and other self-care activities.
- Set clear, consistent limits to provide a sense of security and structure, but allow for exploration within those limits.
- Avoid shaming or ridiculing attempts at independence.
- Facilitate parallel play opportunities.
- Prepare toddlers for changes in routine, and try to maintain established rituals when possible (e.g., bringing a favorite blanket to the hospital).
- Teach sharing, but understand that it is a developing concept.
- Reassure parents that negativism is a normal phase of development and not defiance.
Nursing Insight: Autonomy vs. Shame and Doubt is core conflict. Offer limited, safe choices to foster independence. Avoid power struggles; allow them to do things for themselves.
Temperament
Temperament refers to an individual's innate behavioral style and emotional characteristics. It influences how a toddler interacts with their environment and responds to various stimuli.
While not modifiable, understanding a toddler's temperament helps parents and caregivers adapt their parenting strategies.
Thomas and Chess identified nine characteristics of temperament, often grouped into three broad categories:
- Easy Child: Generally positive mood, adaptable, low or moderate intensity of reactions, regular and predictable biological rhythms. They adapt easily to new situations.
- Difficult Child: Irregular biological rhythms, negative mood, intense reactions, slow to adapt to new situations, and often withdraw from novel stimuli. They tend to be more challenging to parent.
- Slow-to-Warm-Up Child: Low activity level, generally negative mood, low intensity of reactions, adapt slowly to new situations, and may initially withdraw but eventually adapt if given time.
Nine Characteristics of Temperament (Thomas & Chess):
- Activity Level: Degree of physical motion during activity (e.g., high-energy vs. quiet).
- Rhythmicity (Regularity): Predictability of biological functions like hunger, sleep, and elimination.
- Approach/Withdrawal: Initial response to new stimuli, people, or places (e.g., immediate engagement vs. hesitation).
- Adaptability: Ease with which a child adjusts to changes in routine or environment.
- Intensity of Reaction: Energy level of response, whether positive or negative (e.g., loud laughter vs. quiet smile).
- Threshold of Responsiveness: Intensity of stimulation required to evoke a response.
- Quality of Mood: Predominant emotional state (e.g., cheerful vs. serious).
- Distractibility: Ease with which external stimuli can interfere with ongoing behavior.
- Attention Span and Persistence: Length of time an activity is pursued and ability to continue in the face of obstacles.
Nursing Implications for Temperament:
- Assess the toddler's temperament characteristics during health visits.
- Educate parents about temperament as an innate trait, not a reflection of their parenting skills or the child's "badness."
- Help parents understand their child's unique temperament and how to adapt their parenting style to promote a "goodness of fit" between parent and child.
- Suggest strategies for managing challenging temperaments (e.g., for a difficult child, maintain consistent routines, introduce new situations slowly; for a slow-to-warm-up child, allow time for adjustment).
- Validate parental feelings and offer support.
Coping With Concerns Related To Normal Growth And Development
- Toddlerhood is a period filled with developmental "tasks" that can present challenges for both the child and the parents.
- Nurses can provide valuable guidance and strategies for coping with these normal, yet sometimes frustrating, behaviors.
1.1. Toilet Training
Toilet training is a significant developmental milestone influenced by physical and psychological readiness.
- Readiness Signs (usually between 18-30 months):
- Physical Readiness:
- Ability to walk, sit, and squat.
- Has dry periods of at least 2 hours or wakes dry from a nap.
- Has regular, predictable bowel movements.
- Can pull pants up and down.
- Cognitive Readiness:
- Can understand and follow simple directions.
- Can communicate the need to go to the bathroom (verbally or nonverbally).
- Shows curiosity about using the toilet.
- Psychological Readiness:
- Expresses a desire for independence and control.
- Shows interest in the toilet and wants to imitate adults.
- Is not in a period of major stress or transition (e.g., new sibling, moving).
- Has a positive relationship with the parent.
- Physical Readiness:
Nursing Insight: Readiness, not age, is key. Educate parents on physical, cognitive, and psychological readiness cues. Starting too early causes frustration and delay.

- Nursing Interventions/Guidance:
- Patience and Positive Reinforcement: Emphasize patience, consistency, and a positive approach. Praise efforts, not just success.
- Avoid Punishment: Never punish for accidents. This can lead to fear, shame, and delayed training.
- "Readiness" Approach: Stress that training should begin when the child shows readiness, not when the parents are ready or when the child reaches a certain age.
- Equipment: Suggest a child-sized potty chair or a toilet seat insert with a step stool.
- Routine: Establish a consistent routine, such as taking the child to the potty after meals or upon waking.
- Dress: Suggest easily removable clothing.
- Bowel Training First: Often, bowel control is achieved before bladder control. Focus on one at a time.
- Nighttime Training: Nighttime bladder control usually develops after daytime control.
- Dealing with Resistance: If the child resists, stop training for a few weeks and then try again.
- Hygiene: Teach proper wiping and handwashing.
1.2. Sibling Rivalry
Sibling rivalry is a common phenomenon when a new baby enters the family, or even between existing siblings.
- Causes: Competition for parental attention, perceived loss of parental love, jealousy, and developmental stage (egocentricity).
- Manifestations: Regression (e.g., bedwetting, thumb-sucking), aggression towards the sibling, increased negativism, attention-seeking behaviors.
- Nursing Interventions/Guidance:
- Prepare the Toddler: Prepare the toddler for the new baby's arrival well in advance, involving them in preparations.
- Assure Love and Attention: Reassure the toddler of continued love and attention.
- Special Time: Dedicate special one-on-one time with the toddler each day.
- Involve the Toddler: Involve the toddler in the care of the new baby (e.g., fetching diapers, singing songs, helping with feeding).
- Avoid Comparisons: Do not compare siblings.
- Acknowledge Feelings: Validate the toddler's feelings of frustration or anger.
- Manage Aggression: Set clear limits on aggressive behavior.
- Encourage Play: Encourage positive interactions and parallel play.
- Gifts: Present a "gift" from the new baby to the toddler.
1.3. Temper Tantrums
Temper tantrums are common in toddlers and are a normal part of their development, reflecting their struggle between their desire for independence and their limited communication skills and impulse control.
- Causes: Frustration, inability to communicate needs/desires effectively, fatigue, hunger, overstimulation, desire for control/autonomy.
- Manifestations: Crying, screaming, hitting, kicking, throwing objects, breath-holding spells (less common but can occur).
- Nursing Interventions/Guidance:
- Prevention:
- Avoid situations likely to provoke tantrums (e.g., overtired, hungry).
- Offer choices (within limits) to give a sense of control.
- Prepare toddlers for transitions.
- Distraction.
- During a Tantrum:
- Remain Calm: Parents should remain calm and avoid escalating the situation.
- Ignore the Behavior (if safe): If the tantrum is for attention, ignore the behavior as long as the child is safe.
- Time-Out: Use a brief time-out (1 minute per year of age) for destructive or aggressive behavior.
- Safety First: Ensure the child is safe from injury.
- Avoid Arguing/Reasoning: Reasoning during a tantrum is ineffective.
- After a Tantrum:
- Offer comfort once the child has calmed down.
- Discuss the situation briefly and calmly, reinforcing rules.
- Return to normal activity.
- Consistency: Consistent responses from caregivers are key.
- Prevention:
1.4. Negativism
Negativism, characterized by a frequent "no" and resistance to suggestions, is a hallmark of toddlerhood.
- Causes: A natural expression of the toddler's developing autonomy and desire for independence. It's their way of asserting control.
- Manifestations: Saying "no" to everything, refusing to cooperate, doing the opposite of what is asked.
- Nursing Interventions/Guidance:
- Offer Choices: Give toddlers choices that are acceptable to the parent (e.g., "Do you want to wear the blue shirt or the red shirt?" instead of "Put on your shirt").
- Avoid "No" Questions: Phrase requests positively (e.g., "It's time to clean up" instead of "Do you want to clean up?").
- Limit Settings: Set clear and consistent limits to provide structure and security.
- Positive Reinforcement: Praise cooperative behavior.
- Humor and Playfulness: Sometimes, a playful approach can diffuse negativism.
- Patience: Remind parents that this is a normal developmental phase that will pass.
Nursing Insight: "No" is assertion of autonomy. Offer limited choices such as "Do you want the red or blue shirt?" and phrase requests positively to give a sense of control.
1.5. Stress
Toddlers can experience stress, even though they may not be able to articulate it. Significant changes or events can be stressful.
- Stressors: New sibling, moving, parental conflict/divorce, hospitalization, starting childcare, loss of a loved one, significant changes in routine.
- Manifestations: Regression, changes in sleep/eating patterns, increased irritability, clinginess, increased aggression, withdrawal, difficulty with toilet training.
- Nursing Interventions/Guidance:
- Maintain Routine: Whenever possible, maintain consistent routines.
- Predictability: Provide predictability and preparation for changes.
- Reassurance: Offer extra comfort, cuddles, and reassurance.
- Verbalize Feelings: Help the child verbalize feelings (e.g., "You seem sad").
- Play Therapy: Encourage play as a way for the child to express and process stress.
- Parental Support: Support parents in managing their own stress, as parental stress can affect the child.
- Professional Help: Recommend professional help if stress is severe or prolonged.
1.6. Regression
Regression is a temporary return to an earlier developmental stage in response to stress, illness, or changes in routine.
- Causes: New baby, hospitalization, illness, starting a new daycare, toilet training pressure, family conflict.
- Manifestations: Resuming behaviors like thumb-sucking, bedwetting (after being trained), wanting a bottle, increased clinginess, baby talk.
- Nursing Interventions/Guidance:
- Acknowledge and Validate: Acknowledge that the behavior is a normal response to stress.
- Avoid Punishment: Do not punish or shame the child for regressing.
- Provide Reassurance: Offer extra comfort and security.
- Focus on Underlying Cause: Address the underlying stressor if possible.
- Reinforce Age-Appropriate Behaviors: Gently encourage and praise age-appropriate behaviors when the stress subsides.
- Temporary Nature: Reassure parents that regression is usually temporary.
- Gradual Return: Expect a gradual return to previous developmental achievements.
Nursing Insight: Regression is a normal coping mechanism. Do not punish regressive behaviors. Provide extra comfort, address the underlying stressor, and gently encourage age-appropriate behaviors when the stress subsides.
Promoting Optimum Health During Toddlerhood
- Promoting optimal health in toddlers involves ensuring proper nutrition, adequate sleep and activity, good dental hygiene, and robust safety measures to prevent injuries.
1.1. Nutrition
Toddler nutrition is crucial for continued growth and development. Their nutritional needs shift as their growth rate slows, and they transition to a more varied diet.
- Physiological Anorexia: A common developmental phase where toddlers appear to eat very little and become picky eaters. This is normal due to slowed growth and increased focus on other developmental tasks.
- Calorie Needs: Approximately 100 kcal/kg/day, but individual needs vary.
- Dietary Guidelines:
- Three Meals, Two Snacks: Offer three regular meals and two nutritious snacks daily.
- Small Portions: Offer small, age-appropriate portions. Toddlers have small stomachs.
- Variety: Offer a wide variety of foods from all food groups.
- Picky Eaters:
- Do not force-feed.
- Offer new foods repeatedly (it can take 10-15 exposures for acceptance).
- Involve toddlers in food preparation (e.g., washing vegetables).
- Make mealtime pleasant, not a battleground.
- Avoid using food as a reward or punishment.
- Fluid Intake:
- Milk: Whole milk until age 2 for adequate fat for brain development, then reduced-fat milk. Limit milk intake to 16-24 oz (480-720 mL) per day to prevent "milk anemia" (iron deficiency due to excessive milk displacing iron-rich foods).
- Water: Offer water freely between meals.
- Juice: Limit 100% fruit juice to 4-6 oz (120-180 mL) per day, diluted, and offered in a cup, not a bottle. Avoid sugary drinks.
- Iron Deficiency Anemia: Common in toddlers due to excessive milk intake and inadequate iron-rich food consumption.
- Prevention: Introduce iron-fortified cereals and iron-rich foods (meat, poultry, fish, beans, fortified breads).
- Screening: Universal screening for anemia at 12 months.
- Choking Hazards: Avoid small, round, or hard foods that can cause choking:
- Hot dogs (cut lengthwise)
- Grapes (cut into quarters)
- Nuts, seeds
- Popcorn
- Hard candies, gum
- Large chunks of meat or cheese
- Peanut butter (thick smears)
- Nursing Interventions/Guidance:
- Provide anticipatory guidance on normal toddler eating behaviors.
- Educate parents on balanced nutrition, portion sizes, and choking prevention.
- Assess dietary intake during well-child visits.
- Advise on strategies for picky eaters.
- Emphasize family meal times and modeling healthy eating behaviors.
1.2. Vegetarian Diets
Vegetarian diets can be healthy for toddlers if well-planned to ensure adequate intake of essential nutrients.
- Types:
- Lacto-ovo vegetarian: Includes dairy and eggs.
- Lacto vegetarian: Includes dairy but no eggs.
- Vegan: Excludes all animal products.
- Nutrient Concerns (especially for vegans):
- Protein: Ensure adequate intake from legumes, lentils, nuts, seeds, tofu, fortified plant milks.
- Iron: Plant-based iron (non-heme) is less bioavailable. Include iron-rich plant foods (e.g., fortified cereals, spinach, beans, lentils) and pair them with Vitamin C sources to enhance absorption.
- Vitamin B12: Found almost exclusively in animal products. Vegan toddlers must receive B12 supplements or consume B12-fortified foods (e.g., fortified plant milks, nutritional yeast).
- Vitamin D: Fortified foods (plant milks) or supplements.
- Calcium: Fortified plant milks, leafy greens, fortified tofu.
- Zinc: Legumes, nuts, seeds, whole grains.
- Omega-3 Fatty Acids: Flaxseed, chia seeds, walnuts, or algal oil supplements.
- Nursing Interventions/Guidance:
- Assess the type of vegetarian diet and the parents' understanding of nutritional needs.
- Educate parents on potential nutrient deficiencies and how to address them through food choices and supplementation.
- Encourage consultation with a registered dietitian specializing in pediatric nutrition.
- Stress the importance of variety and balanced meal planning.
- Monitor growth closely in vegetarian toddlers.
1.3. Complementary and Alternative Medicine (CAM)
Parents may use CAM therapies for their toddlers. Nurses need to be knowledgeable, non-judgmental, and ensure safety.
- Common CAM therapies: Herbal remedies, homeopathy, chiropractic, acupuncture, massage therapy, dietary supplements (e.g., vitamins, probiotics).
- Considerations for Toddlers:
- Dosage: Dosing for children can be challenging and dangerous, as most CAM products are designed for adults.
- Purity/Safety: Lack of regulation means product purity, potency, and safety are not guaranteed. Contaminants can be present.
- Interactions: Potential for interactions with conventional medications.
- Effectiveness: Many CAM therapies lack scientific evidence of efficacy in children.
- Delayed Conventional Treatment: Reliance on CAM can sometimes delay seeking effective conventional medical care.
- Nursing Interventions/Guidance:
- Open Communication: Ask parents about any CAM therapies they are using or considering. Create an open, non-judgmental environment.
- Education: Provide accurate, evidence-based information about the CAM therapy, including potential benefits, risks, and interactions.
- Safety First: Prioritize the child's safety. Advise against unproven or potentially harmful therapies.
- Collaboration: Encourage parents to discuss CAM use with their healthcare provider to ensure coordinated and safe care.
- "Do No Harm": Emphasize the principle of "do no harm" when discussing CAM.
1.4. Sleep and Activity
Adequate sleep and physical activity are essential for toddler growth, development, and overall health.
- Sleep:
- Duration: Toddlers need approximately 11-14 hours of sleep per 24-hour period, including a daytime nap (usually 1 nap per day by 18 months, lasting 1-3 hours).
- Bedtime Rituals: Consistent bedtime routines (bath, story, quiet play) promote good sleep habits.
- Sleep Problems:
- Night Terrors/Nightmares: Common. Night terrors occur during non-REM sleep, child is usually not fully awake, and doesn't remember. Nightmares occur during REM sleep, child awakens and remembers.
- Resisting Bedtime: Due to desire for autonomy and fear of separation.
- Waking During the Night: May be due to developmental changes, separation anxiety, or habit.
- Nursing Interventions/Guidance for Sleep:
- Advise on consistent sleep schedules and routines.
- Ensure a safe, dark, and quiet sleep environment.
- Address parental concerns about sleep problems, offering strategies like positive reinforcement for staying in bed, brief comfort for night wakings, and distinguishing between night terrors and nightmares.
- Avoid overtiredness, as this makes it harder to fall asleep.
Nursing Insight: Consistent routines are key for sleep. Promote predictable bedtime rituals and sleep schedules to minimize sleep resistance and night wakings.
- Activity:
- Physical Activity: Toddlers are naturally active. They need at least 60 minutes of unstructured active play daily, spread throughout the day.
- Opportunities: Provide opportunities for running, jumping, climbing, throwing, and dancing.
- Screen Time: Limit screen time (TV, tablets, phones) to less than 1 hour per day of high-quality programming, and preferably none for children under 18-24 months. Avoid screens before bedtime.
- Nursing Interventions/Guidance for Activity:
- Promote active, unstructured play.
- Educate on the risks of excessive screen time.
- Encourage outdoor play.
- Advise parents to be role models for active lifestyles.
1.5. Dental Health
Dental health is critical during toddlerhood, as primary teeth are essential for chewing, speech, and maintaining space for permanent teeth.
- Eruption: By 2.5-3 years, most toddlers have a full set of 20 primary teeth.
- Dental Caries (Cavities): Common in toddlers, particularly "early childhood caries" (ECC) or "baby bottle tooth decay," often caused by prolonged exposure to sugary liquids (milk, juice) in bottles, especially at night or for comfort.
- Oral Hygiene:
- Brushing: Begin brushing teeth as soon as the first tooth erupts using a soft-bristled brush.
- Toothpaste: Use a "smear" of fluoridated toothpaste (rice-grain size) for children under 3.
- Parental Responsibility: Parents should brush the toddler's teeth until they develop sufficient dexterity (around 6-7 years).
- Dental Visits: First dental visit by 1 year of age or within 6 months of the first tooth eruption.
- Fluoride: Discuss optimal fluoride intake (water fluoridation, fluoride supplements if water is not fluoridated, professional fluoride varnish).
- Nursing Interventions/Guidance:
- Educate parents on proper oral hygiene practices (brushing, toothpaste use).
- Advise against putting toddlers to bed with bottles containing anything other than water.
- Encourage sipping milk/juice from a cup, not a bottle, and limiting frequency.
- Stress the importance of the first dental visit and regular check-ups.
- Assess for signs of ECC during well-child visits.
1.6. Safety Promotion and Injury Prevention
- Injuries are the leading cause of death and disability in toddlers. Nurses play a crucial role in providing anticipatory guidance for injury prevention. Toddlers' increased mobility, curiosity, and limited understanding of danger put them at high risk.
- Common Injury Types:
- Falls: From stairs, furniture, windows.
- Poisoning: Ingestion of medications, cleaning products, plants.
- Drowning: In bathtubs, toilets, buckets, swimming pools.
- Burns: From hot liquids, electrical outlets, stoves.
- Motor Vehicle Accidents (MVAs): Improper car seat use, lack of restraints.
- Choking/Suffocation: Small objects, food, plastic bags.
- Aspiration: Foreign objects.
- Bodily Damage: Cuts, bruises, animal bites.
- Key Principles of Safety Promotion:
- Anticipatory Guidance: Educate parents before the child reaches a developmental stage where they are at risk for a particular injury.
- Childproofing: Make the home environment safe.
- Supervision: Constant, active supervision is paramount.
- Education: Teach safety rules as the child matures.
- Specific Safety Measures:
- Motor Vehicle Safety:
- Car Seats: Rear-facing car seats until at least 2 years of age or until they reach the maximum height and weight limit for their car seat.
- Always use appropriate car seats, correctly installed, for every ride.
- Children should ride in the back seat.
- Drowning Prevention:
- Never leave a toddler unsupervised in or near water (bathtubs, pools, even shallow water).
- Fence swimming pools with self-latching gates.
- Empty buckets and bathtubs immediately after use.
- Learn CPR.
- Burns:
- Set water heater temperature to less than 120°F (49°C).
- Cover electrical outlets.
- Keep hot foods/liquids out of reach.
- Use back burners on stoves.
- Keep matches/lighters out of reach.
- Install smoke detectors and carbon monoxide detectors.
- Poisoning:
- Store all medications, cleaning products, chemicals, and toxic plants in locked cabinets or out of reach.
- Keep the Poison Control Center number readily available (1-800-222-1222 in the US).
- Never refer to medicine as "candy."
- Falls:
- Install gates at the top and bottom of stairs.
- Secure furniture (dressers, bookshelves) to walls to prevent tipping.
- Supervise closely on playgrounds.
- Window guards on upper-story windows.
- Choking/Suffocation/Aspiration:
- Keep small objects (coins, buttons, batteries, magnets) out of reach.
- Avoid choking hazard foods (see Nutrition section).
- Cut food into small, bite-sized pieces.
- Keep plastic bags away from children.
- Inspect toys for small or broken parts.
- Bodily Damage:
- Secure heavy items.
- Keep sharp objects (knives, scissors) out of reach.
- Supervise interactions with pets.
- Teach "stranger danger" in age-appropriate ways.
- Gun Safety: If guns are in the home, they should be stored unloaded, locked, and separate from ammunition.
- Motor Vehicle Safety:
Nursing Implications for Safety Promotion:
- Conduct thorough safety assessments of the home environment during well-child visits.
- Provide clear, concise, and individualized anticipatory guidance based on the child's developmental stage and family's specific circumstances.
- Use visual aids and demonstrations (e.g., car seat checks).
- Reinforce safety messages at every encounter.
- Empower parents to be proactive in creating a safe environment.
Summary
- The nursing management of the toddler revolves around supporting the family through the predictable "terrible twos" while monitoring for healthy maturation across all domains.
- A significant portion of pediatric nursing care involves helping parents cope with normal developmental hurdles. This includes providing strategies for toilet training, which requires both physical and psychological readiness, and managing the emotional outbursts known as temper tantrums.
- Nurses must educate parents that behaviors like negativism and regression are often healthy responses to stress or the arrival of a new sibling rather than signs of behavioral failure. By reframing these challenges as milestones of independence, the nurse fosters a more patient and effective parenting environment.
- Health promotion during toddlerhood requires a shift toward preventive education. Nutritional counseling is paramount, especially regarding the transition to "table foods" and the management of picky eating habits.
- For families following vegetarian diets or utilizing complementary and alternative medicine, the nurse must ensure that the child's intake remains nutritionally complete, particularly in terms of iron and vitamin B12.
- Sleep hygiene and dental health also emerge as priorities. The nurse should advocate for the "dental home" and the cessation of nighttime bottle-feeding to prevent early childhood caries.
- Safety promotion and injury prevention remain the highest priority, as the toddler's increased mobility and natural curiosity far outpace their cognitive ability to recognize danger. Nurses must be vigilant in educating families about the risks of drowning, poisoning, and falls.
- By integrating evidence-based practice with a deep empathy for the family's daily struggles, the nurse ensures that the toddler moves through this stage with a strong foundation of physical health and a resilient sense of self.
