
Ati med surg proctored exam
Ati med surg proctored exam
Total Questions : 57
Showing 10 questions Sign up for moreA nurse is caring for a client.
Which of the following actions should the nurse take?
Select all that apply.
Explanation
A. Wear an N95 mask when caring for the client: An N95 mask is necessary for airborne infections such as tuberculosis or measles. Pneumonia caused by typical bacteria or viruses is spread by droplets, so a surgical mask is sufficient, not an N95.
B. Place the client in a private room: Clients with pneumonia should be placed in a private room to prevent transmission of infectious droplets to others, especially those who are immunocompromised or at higher risk for respiratory infections.
C. Place the client on droplet isolation precautions: Pneumonia spreads through large respiratory droplets from coughing or sneezing. Droplet precautions include wearing a surgical mask within 3 feet of the client and limiting close contact exposure.
D. Assign client to a negative air pressure room: A negative air pressure room is required for airborne precautions, not droplet infections like pneumonia. It is unnecessary and would reserve specialized rooms for conditions requiring them.
E. Ensure the client wears a mask when outside their room: Having the client wear a surgical mask while leaving the room helps contain respiratory secretions and prevents droplet transmission to others in hallways or procedure areas.
A nurse on a medical-surgical unit is reviewing the electronic health record of a client who is being admitted from the emergency department.
After reviewing the client's EHR, which of the following client's findings require further follow-up by the nurse?
Click to highlight the client's findings that require further follow-up by the nurse. To deselect a finding, click on the finding again.
|
Body System |
Findings |
|
Gastrointestinal |
Client reports abdominal pain as a 9 on a pain scale of 0 to 10. Abdomen is distended and firm. Bowels sounds are distant and hypoactive. |
|
Integumentary |
Skin is warm and dry. Perianal skin is excoriated, and small ulceration is noted. |
|
Fluid balance |
Tenting of skin for 4 seconds is noted. Capillary refill is 2 seconds. Temperature 38.7° C (101.7° F) Mucous membranes are dry. Respiratory rate 20/min |
Explanation
Rationale for Correct Choices:
• Client reports abdominal pain as a 9 on a pain scale of 0 to 10: Severe abdominal pain indicates significant underlying pathology. In the presence of vomiting, distention, and altered bowel sounds, it could reflect obstruction, ischemia, or peritonitis, requiring urgent intervention.
• Abdomen is distended and firm: Distention and firmness suggest accumulation of gas or fluid within the abdomen. This is concerning for bowel obstruction or peritonitis, which can compromise circulation and lead to sepsis if untreated.
• Bowel sounds are distant and hypoactive: Diminished bowel sounds point to decreased peristalsis. In a client with abdominal pain and distention, this strongly suggests obstruction or ileus, requiring prompt diagnostic and therapeutic measures.
• Perianal skin is excoriated, and small ulceration is noted: Frequent diarrhea has led to skin breakdown and ulceration. This not only causes pain and discomfort but also increases the risk of secondary infection, requiring local wound care and protection.
• Tenting of skin for 4 seconds is noted: Delayed skin turgor indicates poor hydration status. Given this client’s vomiting, diarrhea, and low oral intake, this is a strong indicator of fluid volume deficit needing IV replacement.
• Temperature 38.7 °C (101.7 °F): Fever signals the presence of infection. With gastrointestinal complaints, this may be due to bacterial gastroenteritis, abscess formation, or other intra-abdominal infection that warrants further evaluation.
• Mucous membranes are dry: Dry mucous membranes reflect fluid volume depletion. This is consistent with the client’s history of poor intake, vomiting, and diarrhea, and further confirms dehydration.
Rationale for Incorrect Choices:
• Skin is warm and dry: Warm, dry skin suggests adequate peripheral perfusion and does not require follow-up compared to more urgent findings like dehydration and abdominal changes.
• Capillary refill is 2 seconds: A refill time under 3 seconds indicates sufficient peripheral circulation. This finding is within normal limits and does not require additional intervention.
• Respiratory rate 20/min: A respiratory rate within the range of 12–20 breaths/min is considered normal for adults. This shows stable respiratory function and does not require follow-up.
Explanation
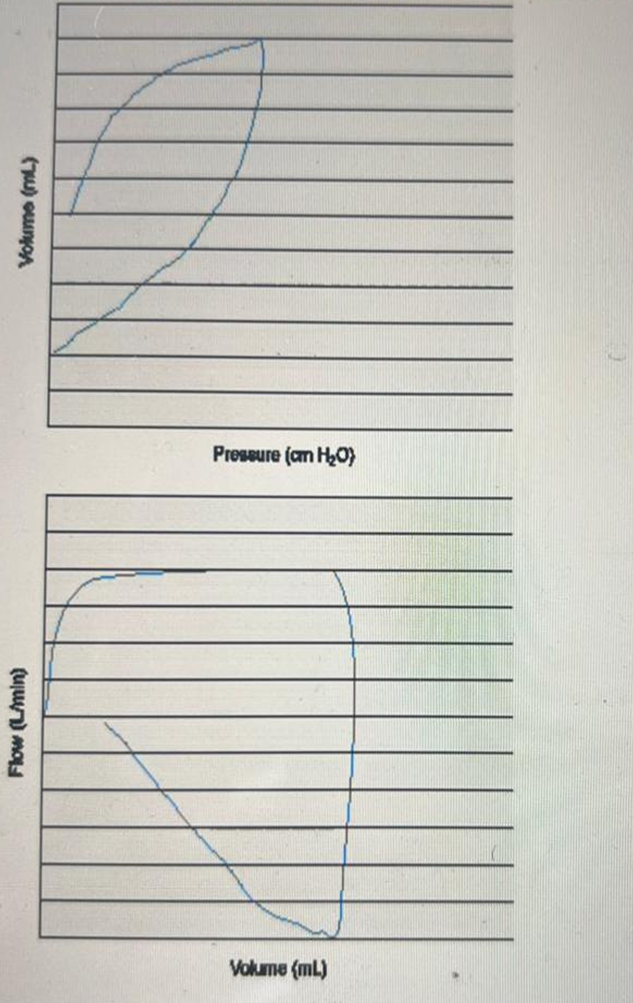
The pressure–volume loop shows a "beaking" pattern (upper inflection point, where the loop flattens and bends back). This indicates overdistention of the alveoli from excessive tidal volume or high inspiratory pressure. The flow–volume loop shows a scooped-out appearance during expiration, which is typical of airflow obstruction such as COPD or asthma. These loops are most consistent with obstructive lung disease with overdistention such as in COPD.
A nurse is creating a plan care for a client who requires suture removal. Which of the following actions should the nurse plan to take?
Explanation
A. Pull the visible part of the suture through the underlying tissue: Pulling the external portion of the suture through the tissue can introduce surface bacteria into the wound. This increases the risk of infection and should be avoided.
B. Cleanse the wound with sterile water prior to removing the sutures: Wounds are typically cleansed with sterile normal saline or an antiseptic solution, not sterile water. Normal saline is isotonic and safe for wound irrigation, whereas sterile water can damage tissue.
C. Cut the sutures as close to the skin as possible: Cutting close to the skin ensures only the buried portion of the suture is pulled through the tissue, reducing contamination and promoting proper healing.
D. Remove the sutures in a consecutive order: Sutures are usually removed every other one first to prevent wound dehiscence. Removing them consecutively can place stress on the wound edges and increase the risk of reopening.
A nurse manager is teaching a group of newly licensed nurses about which procedures are within their scope of practice. Which of the following examples should the nurse include in the teaching?
Explanation
A. Insertion of an endotracheal tube: Endotracheal intubation is outside the scope of practice for registered nurses. This procedure is performed by providers such as anesthesiologists, respiratory therapists, or specially trained advanced practice nurses.
B. Monitoring a continuous intra-arterial infusion of a thrombolytic medication: Nurses are responsible for closely monitoring patients receiving high-risk infusions. This includes assessing for complications such as bleeding, changes in vital signs, and effectiveness of therapy, which falls within an RN’s scope of practice.
C. Placement of nylon sutures: Suturing is a procedure performed by providers or advanced practice nurses, not registered nurses. Performing sutures is outside the RN’s scope of practice in most care settings.
D. Administering a bolus dose of medication through an epidural catheter: Epidural bolus administration requires advanced training and is usually limited to anesthesiologists, certified registered nurse anesthetists (CRNAs), or pain specialists.
A nurse is caring for a client who had a stroke and is immobile. Which of the following actions should the nurse take to maintain the client's skin integrity?
Explanation
A. Insert an indwelling urinary catheter: Indwelling catheters increase the risk of urinary tract infections and are not recommended solely for immobility. Managing incontinence with skin care and barrier products is safer for preserving skin integrity.
B. Use an alcohol-free barrier product: Alcohol-free barrier products protect the skin from moisture, friction, and irritation without causing dryness. This helps maintain skin integrity, especially in clients who are immobile and at high risk for breakdown.
C. Reposition the client every 4 hr: Immobile clients should be repositioned at least every 2 hours, not every 4. Prolonged pressure over bony areas can rapidly lead to pressure injuries if turning is delayed.
D. Massage the skin over bony prominences: Massaging over bony prominences can damage fragile tissue and worsen the risk of pressure injury. Instead, gentle repositioning and cushioning should be used to protect the skin.
A nurse receives a telephone call from a client's family member, who asks the nurse for an update on the client's condition. Which of the following actions should the nurse take to maintain the client's confidentiality?
Explanation
A. Request additional information about the caller's relationship to the client: Even if the caller provides details about their relationship, this does not guarantee that the client has authorized disclosure. Verifying identity alone is not sufficient to maintain confidentiality.
B. Provide a general update about the client's condition over the telephone: Giving any medical information, even general, without the client’s consent is a breach of confidentiality and violates HIPAA regulations.
C. Refer the family member to the client's provider for the update: Referring the caller to the provider still risks confidentiality concerns if the client has not given explicit permission. Authorization must come from the client before anyone shares details.
D. Encourage the family member to contact the client directly for information: This maintains client confidentiality by ensuring that health information is shared only if the client chooses to disclose it. It protects privacy while respecting the client’s autonomy.
A nurse is planning an in-service about foot care for a group of clients who have peripheral neuropathy. Which of the following information should the nurse include?
Explanation
A. Apply foot cream between the toes: Moisturizing between the toes can create a warm, moist environment that promotes fungal or bacterial infections. Foot cream should be applied to the tops and bottoms of the feet, avoiding spaces between the toes.
B. Use a pumice stone to soften calluses: Using a pumice stone can cause skin breaks or ulcers in clients with peripheral neuropathy due to reduced sensation. Callus management should be performed by a healthcare professional to prevent injury.
C. Inspect the feet daily using a mirror: Daily inspection helps identify cuts, blisters, or infections early, especially since clients with peripheral neuropathy may not feel injuries due to decreased sensation. Using a mirror allows visualization of hard-to-see areas such as the soles.
D. Round the toenail edges when clipping: Toenails should be trimmed straight across to prevent ingrown nails and reduce the risk of infection. Rounding the edges can increase the likelihood of nail problems in clients with neuropathy.
A nurse is performing a family assessment for a client who has recently developed paraplegia following a stroke. Which of the following actions should the nurse take first?
Explanation
A. Determine how the client views the concept of a family: Understanding the client’s personal definition of family helps the nurse identify who the client considers significant for support and involvement in care planning, ensuring a patient-centered approach.
B. Identify how culture influences family functioning: Cultural influences are important in understanding family dynamics, but assessing the client’s perception of family comes first. Culture shapes interactions, but only after the nurse knows who the family members are from the client’s perspective.
C. Determine if the client has an external support system: Knowing about external supports is valuable, but this information is secondary to identifying the client’s family structure and relationships. Support systems can be assessed once the family context is clear.
D. Identify how the family deals with unexpected health changes: Assessing coping strategies is necessary for planning interventions, but it should occur after the nurse has first established who comprises the client’s family and understands their roles.
A nurse is teaching a client to manage stress by using progressive relaxation techniques. Which of the following statements by the client indicates an understanding of the teaching?
Explanation
A. "I should breathe normally while I am performing this relaxation technique.": Progressive relaxation often involves focused, deep, and controlled breathing to enhance muscle relaxation. Simply breathing normally may not maximize the effectiveness of the technique.
B. "I should imagine myself in a peaceful, garden-like setting as I begin.": Visualizing a calming scene is a technique used in guided imagery, not progressive muscle relaxation. While relaxation may result, this reflects a different stress-reduction method.
C. "I'll compare the sensations I feel when I tense my muscles to what I feel when I relax them.": Progressive relaxation involves systematically tensing and then relaxing specific muscle groups while focusing on the contrast in sensations.
D. "I'll use a series of stretches when I practice this technique.": Stretching is part of physical exercise routines and differs from progressive relaxation. The focus in progressive relaxation is on controlled tension and release of muscle groups, not performing stretches.
You just viewed 10 questions out of the 57 questions on the Ati med surg proctored exam Exam. Subscribe to our Premium Package to obtain access on all the questions and have unlimited access on all Exams. Subscribe Now

