
Ati RN Fundamentals 2023 proctored exam
Ati RN Fundamentals 2023 proctored exam
Total Questions : 69
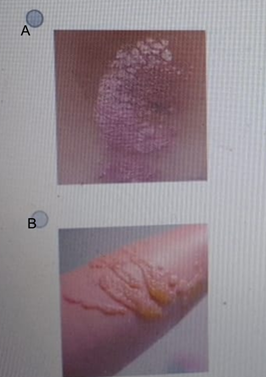
Showing 10 questions Sign up for moreA nurse is assessing a client who is receiving treatment for psoriasis. Which of the following images depicts what the nurse should expect to observe?

Explanation
A. This image shows well-demarcated, erythematous plaques covered with silvery-white scales—classic features of plaque psoriasis. These lesions typically appear on extensor surfaces like the elbows, knees, and scalp, and may itch or crack.
B. This image shows a yellow crusting lesion which suggests impetigo or a secondary skin infection, not psoriasis. Impetigo typically presents with honey-colored crusts, caused by bacterial infection, usually. Psoriasis lesions are usually dry and scaly, not moist or oozing.
C. This image shows red bumps on arm suggesting an allergic reaction, folliculitis, or possibly contact dermatitis. These are small papules often scattered or in clusters, and do not have the thick scaling seen in psoriasis.
D. The fourth image shows linear striae-like marks likely striae distensae (stretch marks), unrelated to psoriasis. Stretch marks are atrophic, linear scars typically due to skin stretching from growth or weight changes. They lack inflammation, plaques, and scale—all key signs of psoriasis.
A nurse is completing discharge teaching about ostomy care with a client who has a new stoma. Which of the following instructions should the nurse include in the teaching? (Select all that apply.)
Explanation
A. "Empty the ostomy pouch when it becomes one-third full of contents.": It is important to empty the ostomy pouch when it is about one-third full to prevent leakage and pressure on the stoma. This helps avoid skin irritation and maintain comfort.
B. "Expect the stoma to turn a purple-blue color as it heals.": A stoma should be a reddish-pink color. A purple or blue color indicates poor circulation and may signal complications such as ischemia, which requires immediate attention.
C. "Cut the opening of the pouch an inch larger than the stoma.": The opening of the ostomy pouch should be cut about one-quarter to one-half inch larger than the stoma to prevent irritation or pressure on the stoma. This ensures a good fit and reduces risk of skin damage.
D. "Place a piece of gauze over the stoma while changing the pouch.": Placing gauze over the stoma during pouch changes protects the skin around the stoma fromcontact with stooland absorbs any drainage.
E. "Use povidone-iodine to clean around the stoma.": Povidone-iodine is too harsh for cleaning the stoma area and may cause skin irritation. The recommended cleaning solution is warm water and mild soap, followed by proper drying, to avoid skin damage and infection.
A nurse is caring for a client who has a chest tube with a closed drainage system. Which of the following actions should the nurse take?
Explanation
A. Milk the chest tube at least three times a day: Milking is generally not recommended as it can increase intrathoracic pressure and damage lung tissue. It should only be done with a provider’s order and specific indication.
B. Empty the drainage collection chamber when full: The collection chamber is a closed system and should not be emptied. When full, the entire drainage unit should be replaced to maintain sterility.
C. Ensure intermittent bubbling is present in the water seal chamber: Intermittent bubbling in the water seal chamber is expected during expiration or coughing, indicating air leaving the pleural space. However, continuous bubbling may suggest an air leak and requires evaluation.
D. Clamp the chest tube when transferring the client from bed to the chair: Clamping the tube is contraindicated during transport, as it can cause tension pneumothorax. The system should remain unclamped and below chest level.
A nurse is caring for a client who is immobile. Which of the following interventions should the nurse plan to take to prevent plantar flexion contractures?
Explanation
A. Prop the feet up: Proping the feet up may not be effective in preventing plantar flexion contractures, as it does not provide sustained support to keep the feet in a neutral position. Plantar flexion can still occur with this position.
B. Apply an abduction pillow to the legs: An abduction pillow is used to keep the hips in a neutral position, not to prevent plantar flexion contractures. It is useful for preventing hip contractures but not specifically for the feet.
C. Use a trochanter roll: A trochanter roll helps prevent external rotation of the hip joint, not plantar flexion of the feet. It is used for positioning to prevent hip complications, but it does not address foot position or contracture prevention.
D. Use foot splints: Foot splints are designed to keep the feet in a neutral or dorsiflexed position, preventing the toes from pointing downward (plantar flexion). This is the most effective intervention to prevent plantar flexion contractures in an immobile client.
A nurse is caring for an adult client who requires nasopharyngeal suctioning. Which of the following actions should the nurse take?
Explanation
A. Set the suction device to 120 mm Hg: For nasopharyngeal suctioning in adults, the suction pressure should typically be set between 100 and 120 mm Hg to prevent injury to the mucous membranes while effectively clearing secretions.
B. Apply suction to the catheter during insertion: Suction should not be applied during insertion of the catheter, as this can cause trauma to the mucous membranes. Suctioning should only occur when the catheter is in the appropriate position and being withdrawn.
C. Have the client tuck his chin to his chest during suctioning: The client should not tuck the chin to the chest during suctioning. Instead, the client should be asked to either cough or breathe normally. Tucking the chin may obstruct the airway and make suctioning difficult.
D. Apply a petroleum-based lubricant to the catheter: Petroleum-based lubricants should not be used as they can cause a fire hazard when oxygen is present. Instead, a water-soluble lubricant should be applied to the catheter if needed.
A nurse is preparing to remove an indwelling urinary catheter from a client. In what order should the nurse perform the following steps? (Move the steps into the box on the right, placing them in the order of performance. Use all the steps.)
Explanation
B. Don clean gloves: The nurse should first don clean gloves to ensure proper hygiene and to reduce the risk of infection during the procedure. This protects both the client and the nurse from any potential contamination.
E. Attach the syringe to the balloon injection port: After gloves are on, the next step is to attach the syringe to the balloon injection port of the catheter. This is the part where sterile fluid (usually saline) was used to inflate the balloon that keeps the catheter in place.
C. Withdraw the solution from the balloon: Once the syringe is attached, the nurse slowly withdraws the fluid from the balloon. This is necessary to deflate the balloon, which allows the catheter to be removed easily and without causing injury to the urethral canal.
A. Slowly pull the catheter out of urethral canal: After the balloon is deflated, the nurse gently and slowly pulls the catheter out of the urethral canal. This should be done carefully to avoid causing trauma to the urethra and surrounding tissues. The catheter should be removed in a smooth, controlled motion.
D. Dry the perineal area: After the catheter is removed, the nurse should clean and dry the perineal area to ensure hygiene. This step helps prevent skin irritation and infection after the catheter removal, ensuring that the area is properly cared for and free of moisture.
A nurse is planning care for a client who has contact precautions in place. Which of the following actions should the nurse plan to take when removing soiled linens from the client's room?
Explanation
A. Double-bag the linens: Double-bagging is no longer a standard requirement unless the outside of the primary bag is visibly soiled or the bag is punctured. Modern infection control guidelines focus on the integrity of a single, sturdy, leak-proof bag to reduce waste and cost.
B. Rinse the linens prior to removing them from the client's room: Rinsing the linens is not required when removing soiled linens. The main concern is preventing contamination, and double-bagging ensures that the linens are safely contained.
C. Tie the linens' bag securely at the top: The primary goal of isolation protocol is to contain the pathogen within the designated "dirty" area. By tying the bag securely, the nurse ensures that no contaminated fluid or air is released as the bag is moved through the hallways of the facility. Standard practice requires placing linens in a leak-proof laundry bag labeled for biohazardous or contaminated materials.
D. Wear sterile gloves when handling the linens: Sterile gloves are not necessary for handling soiled linens in contact precautions. Clean gloves are sufficient to handle linens. Sterile gloves are typically used for invasive procedures, not for routine linen handling.
A nurse is preparing to administer a medication to a client for the first time. Which of the following actions should the nurse take to help ensure safe medication administration?
Explanation
A. Read the medication label twice prior to administration: Best practice requires reading the label three times (when retrieving, preparing, and before administering), so reading it only twice is insufficient for safety.
B. Ask the client if they have ever taken a similar medication: While helpful, this does not replace the need for the nurse to verify the medication's action, side effects, and interactions independently.
C. Use one patient identifier prior to medication administration: Safe practice requires using two patient identifiers (e.g., name and date of birth), so using only one is inadequate and unsafe.
D. Access the online drug formulary for an unfamiliar medication: This ensures the nurse understands the medication's purpose, dosage, side effects, and contraindications, which is critical for safe first-time administration.
A nurse in a postpartum clinic is caring for a client who has returned for their 6-week postpartum visit. The client states emphatically, "I hate when the baby cries, and I can't get them to stop." Which of the following statements should the nurse respond with?
Explanation
A. "You should try putting the baby in a carrier so you can take a walk when they start crying.": This response may not address the client's emotional frustration. It's important to first listen and understand the full context before offering advice.
B. "Tell me more about what is going on when the baby starts crying.": This response shows empathy and invites the client to share more about their experience. It allows the nurse to better understand the situation and provide support or guidance tailored to the client’s concerns.
C. "Many parents have told me it gets better when the baby is about 3 months old.": It's important to explore the client’s current experience and feelings rather than assuming their situation will improve without validating their concerns.
D. "As a new parent, you should be enjoying your time with the baby.": This statement may come across as judgmental as it implies the client should be feeling something different. It is important to acknowledge and validate the client's feelings.
A nurse is caring for a client who was administered more than the prescribed dose of a medication. Which of the following actions should the nurse take first?
Explanation
A. Notify the primary care provider: Notifying the provider is important, but first, the nurse should assess the client’s condition by obtaining vital signs. This helps determine if immediate intervention is needed, like administering antidotes or treatments.
B. Obtain the client's vital signs: The first step is assessing the client’s physical status by checking vital signs. This helps identify signs of toxicity or immediate adverse effects from the overdose, guiding further actions.
C. Educate the client about potential adverse effects: Education is important, but it’s not the first priority in the case of an overdose. The nurse should first focus on assessing and stabilizing the client before providing information on potential adverse effects.
D. Complete an incident report: While an incident report is necessary, it is not the immediate priority. The nurse must first ensure the client’s safety and health by assessing and managing the overdose.
You just viewed 10 questions out of the 69 questions on the Ati RN Fundamentals 2023 proctored exam Exam. Subscribe to our Premium Package to obtain access on all the questions and have unlimited access on all Exams. Subscribe Now

