
Med Surg 2 Proctored Exam
Med Surg 2 Proctored Exam
Total Questions : 85
Showing 10 questions Sign up for moreAfter the nurse receives report, which client should the nurse assess first?
Explanation
A. Client who is experiencing hallucinations and extreme anxiety after the use of marijuana: While hallucinations and anxiety require monitoring and support, they are generally not immediately life-threatening. These symptoms can cause distress but do not pose an acute risk of cardiovascular collapse or respiratory failure.
B. Client with a history of alcohol use complaining of insomnia and diaphoresis: These are early withdrawal symptoms that can progress to more severe complications such as delirium tremens. Although this client requires timely assessment and monitoring, the current presentation is less immediately critical compared to acute cardiovascular instability.
C. Client who has a respiration rate of 14 after overdosing on oxycodone (OxyContin): A respiratory rate of 14 breaths per minute is within normal limits, indicating that the client is currently maintaining adequate ventilation. Continuous monitoring is necessary for opioid overdose, but the client is more stable than those exhibiting severe hemodynamic compromise.
D. Client admitted with cocaine use who has an irregular heart rate of 142 beats/minute and a BP 186/92 mmHg: This client demonstrates signs of acute cardiovascular instability due to stimulant toxicity, including severe hypertension and tachyarrhythmia. These findings place the client at immediate risk for life-threatening complications such as myocardial infarction, stroke, or cardiac arrest, making this client the highest priority for immediate intervention.
The nurse is caring for a client who has been diagnosed with peptic ulcer disease. For Which complication would the nurse monitor?
Explanation
A. Dyspepsia: Dyspepsia, or indigestion, is a common symptom of peptic ulcer disease (PUD) but is not considered a complication. It reflects irritation or inflammation of the gastric or duodenal mucosa rather than a severe pathological outcome requiring urgent intervention.
B. Upper gastrointestinal (GI) bleeding: Upper GI bleeding is a serious and common complication of PUD. Ulceration erodes the gastric or duodenal mucosa and can penetrate blood vessels, leading to hematemesis or melena. This can result in hypovolemia, anemia, and shock if not promptly identified and treated, making vigilant monitoring for signs of bleeding essential.
C. Gastric cancer: Although chronic H. pylori infection and long-standing ulcers can increase gastric cancer risk, malignancy is a less common and long-term risk rather than an immediate complication of PUD. Regular monitoring may be indicated in high-risk clients but it is not the acute complication the nurse would prioritize.
D. Large bowel obstruction: Large bowel obstruction is not associated with PUD, as ulcers occur in the stomach or duodenum. Obstruction typically arises from colonic tumors, strictures, or adhesions, making this an unrelated complication in peptic ulcer disease.
The nurse assesses a client who has a possible gastritis. Which assessment findings indicates that, the client has chronic gastritis? (Select all that applies).
Explanation
A. Intolerance of fatty foods: Chronic gastritis can impair digestive enzyme production and reduce gastric acid secretion, leading to difficulty digesting fats. Clients often report bloating, fullness, or discomfort after consuming fatty meals, which is a common manifestation of long-term mucosal inflammation.
B. Dyspepsia: Dyspepsia, including epigastric discomfort, burning, or gnawing pain, is a hallmark symptom of chronic gastritis. It occurs due to ongoing irritation and inflammation of the gastric mucosa, often exacerbated by certain foods or stress, and persists over weeks to months.
C. Nausea and vomiting: While nausea and vomiting are common in acute gastritis due to sudden mucosal irritation, they are less prominent or intermittent in chronic gastritis. Chronic gastritis often presents with more subtle symptoms rather than acute emesis episodes.
D. Anorexia: Chronic inflammation of the stomach lining can lead to decreased appetite, early satiety, and overall reduced food intake. Anorexia is a characteristic finding in chronic gastritis and may contribute to weight loss over time.
E. Pernicious anemia: Pernicious anemia occurs in chronic gastritis, particularly the autoimmune type, due to atrophy of parietal cells and decreased intrinsic factor production. This results in impaired vitamin B12 absorption, leading to megaloblastic anemia and neurological complications.
The nurse is caring for a client who has frequent gastric pain and dyspepsia. Which procedure would the nurse expect the health care provider to order to make an accurate diagnosis?
Explanation
A. Esophagogastroduodenoscopy (EGD): EGD is the gold standard diagnostic procedure for evaluating clients with frequent gastric pain and dyspepsia. It allows direct visualization of the esophagus, stomach, and duodenum, enabling the detection of gastritis, ulcers, tumors, or other mucosal abnormalities. Additionally, EGD permits biopsy for histopathological examination, which is critical for identifying Helicobacter pylori infection or malignancy.
B. Abdominal arteriogram: An abdominal arteriogram is an imaging study that evaluates the blood vessels of the abdomen and is primarily used to detect vascular abnormalities such as aneurysms or stenosis. It does not provide information about the gastric mucosa or detect the underlying causes of dyspepsia, making it unsuitable for this clinical scenario.
C. Magnetic resonance imaging (MRI): MRI provides detailed images of soft tissue structures but is not routinely used for evaluating mucosal lesions of the stomach or duodenum. While it can detect masses or structural abnormalities, it lacks the sensitivity to identify subtle mucosal inflammation or ulcers that cause dyspepsia.
D. Nuclear medicine scan: Nuclear medicine scans, such as gastric emptying studies or liver-spleen scans, assess organ function rather than provide direct visualization of mucosal surfaces. They are not typically used to diagnose the cause of gastric pain or dyspepsia and are less accurate than EGD for detecting gastritis or peptic ulcers.
The nurse is teaching a client who has been treated for acute gastritis. What statement by the client indicates a need for further teaching?
Explanation
A. "I should drink wine occasionally instead of every night": Reducing alcohol intake is critical for managing gastritis because ethanol irritates the gastric mucosa and increases gastric acid secretion, delaying mucosal healing. Occasional consumption may be permissible for some clients, but moderation is essential to prevent recurrence of inflammation.
B. "I should decrease my intake of caffeinated drinks, especially coffee": Caffeine stimulates gastric acid secretion and can exacerbate symptoms of gastritis, such as epigastric pain and dyspepsia. Limiting coffee, tea, and other caffeinated beverages is a recommended non-pharmacologic intervention to allow mucosal healing and reduce symptom recurrence.
C. "I can continue smoking cigarettes which is better than chewing tobacco": Both smoking and smokeless tobacco negatively affect gastric mucosal integrity. Nicotine increases gastric acid production, reduces bicarbonate secretion, and impairs mucosal blood flow, which delays healing and increases the risk of ulceration. Continuing smoking indicates a misunderstanding of risk factors for gastritis and requires further teaching.
D. "I will take acetaminophen instead of aspirin when I have a headache": Aspirin and other NSAIDs inhibit prostaglandin synthesis, which reduces the protective mucus layer of the stomach and increases the risk of gastritis and peptic ulceration. Acetaminophen does not have this effect on the gastric mucosa, making it a safer alternative for pain management.
A nurse is caring for several clients at risk for shock. Which laboratory value requires the nurse to communicate with the primary health care provider?
Explanation
A. Lactate: 5.4 mg/dL: An elevated lactate level is a critical indicator of tissue hypoperfusion and anaerobic metabolism, often associated with sepsis or other forms of shock. A level of 5.4 mg/dL suggests significant hypoxia at the cellular level. Elevated lactate requires prompt communication with the provider to initiate rapid assessment and interventions.
B. White blood cell count: 11,000/mm³ (11 x 10³/µL): A WBC count of 11,000 is slightly above the normal adult range (4,500–11,000/mm³). While it may indicate early infection or stress response, it is not immediately critical in the context of shock and does not require urgent notification by itself. Trends and associated clinical signs guide further action.
C. Sodium: 150 mEq/L (150 mmol/L): Mild hypernatremia may occur due to dehydration or fluid shifts. Although it warrants monitoring and correction, it is not an immediate life-threatening value in the acute setting of shock compared with lactate, which directly reflects tissue perfusion.
D. Creatinine: 0.9 mg/dL: A creatinine of 0.9 mg/dL is within normal limits (approximately 0.6–1.3 mg/dL for adults) and indicates normal kidney function. This value does not require urgent intervention in a client at risk for shock.
The new nurse reads a client has a wound "healing by second intention" and ask what that means. Which description by the charge nurse is most accurate?
Explanation
A. "The wound was stapled together after an infection was cleared up": This describes primary intention healing, where wound edges are surgically approximated after cleaning or debridement. Stapling or suturing is not part of second-intention healing.
B. "The wound is an open cavity that will fill in with granulation tissue": Second-intention healing occurs when a wound is left open due to tissue loss, contamination, or infection risk. The wound gradually fills with granulation tissue, contracts, and epithelializes over time. This process allows natural healing without suturing.
C. "The wound edges have been approximated and stitched together": This describes primary intention healing, not second intention. Suturing or closing the wound edges accelerates healing but does not involve open wound granulation, so this description is inaccurate.
D. "The wound was contaminated by debris and can't be closed at all": While second-intention wounds may involve contamination or tissue loss, they are capable of healing naturally through granulation and epithelialization. The statement implies the wound cannot heal, which is incorrect; second-intention wounds do heal, albeit more slowly and with a higher risk of scarring.
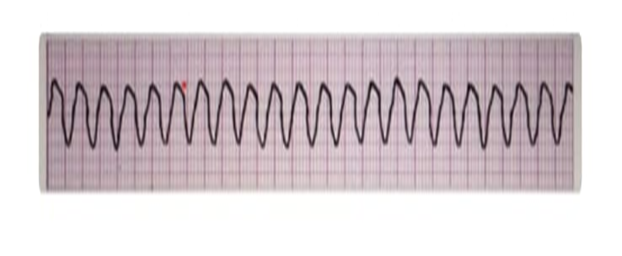
What would be the priority intervention for the care of the client who is pulseless and has the following rhythm on the monitor?
Explanation
A. CPR: Cardiopulmonary resuscitation is essential for maintaining circulation in a pulseless client and should be started immediately; however, CPR alone does not treat the underlying lethal arrhythmia. It serves as supportive care while definitive interventions, like defibrillation, are prepared.
B. Defibrillator: Defibrillation is the priority intervention for pulseless ventricular tachycardia because this is a shockable rhythm. Immediate delivery of an unsynchronized electrical shock can depolarize the myocardium, terminate the arrhythmia, and allow the heart’s natural pacemaker to restore an effective rhythm, significantly increasing the chance of survival.
C. Cardioversion: Synchronized cardioversion is used for unstable, but still perfusing, ventricular tachycardia or other tachyarrhythmias. In a pulseless client, synchronization is unnecessary and would delay life-saving treatment.
D. Amiodarone 300 mg IV bolus. Amiodarone 150 mg bolus if needed: Antiarrhythmic medication like amiodarone can be used as an adjunct after defibrillation and CPR if the rhythm persists. It is not the first-line priority in pulseless ventricular tachycardia because immediate defibrillation is needed to restore circulation.
A 59-year-old client is brought into the emergency room with complaints of chest pain. The client states that the pain is crushing, constrictive pressure that is not relieved with position change. He states that the pain started 3 hours ago in the middle of his chest and radiates down his left arm. The client has a history of diabetes, asthma, and hypertension.
- Temperature: 99
- Blood Pressure: 138/72
- Heart Rate: 106
- Respiration: 19
- ECG: ST segmented depression
- Troponin: Negative
The client is given medication for his unstable angina. Soon after, the client states that he is having difficulty breathing with audible wheezing heard on auscultation. Which of the following is most likely responsible for the symptoms experience by this client?
Explanation
A. Nitroglycerin: Nitroglycerin primarily causes vasodilation of coronary arteries to relieve ischemic chest pain. Common side effects include headache, hypotension, and dizziness, but it does not typically cause bronchospasm or wheezing. The client’s acute respiratory distress is unlikely to be caused by nitroglycerin.
B. Heparin: Heparin is an anticoagulant used to prevent thrombus formation in unstable angina or myocardial infarction. Its adverse effects include bleeding and heparin-induced thrombocytopenia. Heparin does not cause bronchospasm or wheezing, so it is unlikely to cause the client’s respiratory symptoms.
C. Morphine: Morphine is an opioid analgesic used for pain management in acute coronary syndromes. Side effects include respiratory depression, hypotension, and sedation. While morphine can affect respiration, it does not usually produce wheezing or trigger bronchospasm in asthmatic clients.
D. Propranolol: Propranolol is a non-selective beta-adrenergic blocker. In clients with asthma, non-selective beta blockers can block beta-2 receptors in the lungs, causing bronchoconstriction, wheezing, and respiratory distress. Given this client’s history of asthma, propranolol is the most likely cause of the acute dyspnea and audible wheezing, making it the responsible medication.
A client was admitted to the intensive care unit after having an abdominal aortic aneurism resection. The client's cardiac monitor shows a heart rate of 110. The clients hemodynamic monitoring shows a central venous pressure (CVP): 1 mmHg and a pulmonary Arterial Wedge Pressure (PAWP): 3 mmHg. Which health care provider order would the nurse anticipate receiving?
Explanation
A. Decrease IV Fluids to 75 mL/hr and recheck hemodynamic parameters: Decreasing IV fluids in a client with hypotension and low preload (CVP 1 mmHg, PAWP 3 mmHg) would worsen hypovolemia and decrease cardiac output further. Reducing fluid administration is inappropriate because the client shows signs of volume depletion and intravascular hypovolemia.
B. Administer furosemide (Lasix) 20 mg IVP: Furosemide is a loop diuretic used to reduce fluid overload. Administering it to a client with low CVP and PAWP could precipitate severe hypotension, decrease perfusion to vital organs, and exacerbate postoperative shock. This intervention is contraindicated in low preload and tachycardia due to volume depletion.
C. Administer 0.9% Normal Saline @ 150 mL/hr: The client’s low CVP (1 mmHg), low PAWP (3 mmHg), and tachycardia (HR 110) indicate hypovolemia or inadequate circulating volume after abdominal aortic aneurysm surgery. Administering isotonic saline helps restore intravascular volume, improve preload, and optimize cardiac output, making this appropriate.
D. Monitor hemodynamic monitoring parameters again in one hour: Continuous monitoring is essential, but solely waiting without intervening would delay treatment for hypovolemia. Immediate volume replacement takes priority over passive monitoring to prevent hypotension-related complications, organ hypoperfusion, and shock.
You just viewed 10 questions out of the 85 questions on the Med Surg 2 Proctored Exam Exam. Subscribe to our Premium Package to obtain access on all the questions and have unlimited access on all Exams. Subscribe Now

