Acquired Cardiovascular Disorders: Acute Rheumatic Fever
Lessons
Notes Highlighting is available once you sign in. Login Here.
Objectives
- Analyze the relationship between Group A Beta-Hemolytic Streptococcal (GABHS) pharyngeal infections and the subsequent autoimmune development of acute rheumatic fever (ARF).
- Apply the Revised Jones Criteria accurately to differentiate major and minor manifestations for diagnosing primary and recurrent episodes of ARF.
- Identify key clinical manifestations of ARF, focusing on carditis, migratory polyarthritis, Sydenham chorea, erythema marginatum, and subcutaneous nodules.
- Interpret diagnostic findings, including anti-streptolysin O (ASO) titers, acute-phase reactants (ESR, CRP), and echocardiography, to confirm a diagnosis and assess carditis severity.
- Outline the therapeutic management for ARF, focusing on antibiotic eradication therapy, anti-inflammatory medications, and supportive care for chorea and heart failure.
- Develop a comprehensive nursing care plan prioritizing bed rest, pain management for joint pain, neurological safety for chorea, and monitoring for cardiac decompensation.
- Formulate a long-term secondary prevention strategy including appropriate choices, dosages, and duration of prophylactic antibiotic therapy to prevent recurrent ARF and chronic rheumatic heart disease (RHD).
Introduction
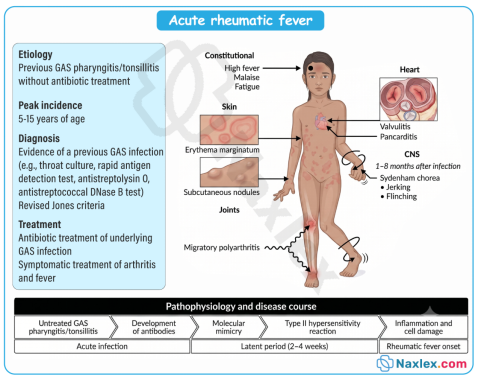
- Acute rheumatic fever (ARF) is a multi-system, nonsuppurative inflammatory disease that occurs as a delayed sequela to an untreated or inadequately treated pharyngeal infection caused by Group A Beta-Hemolytic Streptococcus (GABHS), specifically Streptococcus pyogenes.
- Unlike direct bacterial infections where pathogens tissue-invade local structures, ARF is a classic example of an autoimmune reaction driven by molecular mimicry. The body's immune system, while attempting to eliminate the streptococcal bacteria, mistakenly mounts an attack against its own healthy tissues due to structural similarities between bacterial antigens and human proteins.
- This inflammatory storm target-seeks specific organ systems, predominantly affecting the heart, joints, central nervous system, skin, and subcutaneous tissues.
- Although the manifestations in the joints, skin, and brain are typically transient and resolve without permanent damage, the impact on the heart can be profound and permanent.
- Carditis, or inflammation of the heart tissue, can involve the endocardium, myocardium, and pericardium (pancarditis).
- Acute valvular inflammation can progress over years or decades into chronic rheumatic heart disease (RHD), characterized by permanent valvular scarring, deformity, and subsequent heart failure.
- From a nursing perspective, patients presenting with ARF require vigilant, holistic care. Because ARF primarily strikes school-aged children and young adults, the psychological and physical impact can be severe.
- The nurse plays an indispensable role in recognizing early signs of cardiac stress, managing the extreme discomfort of migratory polyarthritis, and implementing strict safety measures for the involuntary movements of Sydenham chorea.
- Beyond acute stabilization, the nurse serves as a critical educator, ensuring families understand the absolute necessity of long-term secondary antibiotic prophylaxis to safeguard the heart from devastating recurrent attacks.
Epidemiology, Etiology, Risk Factors, And Pathophysiology
Epidemiology
- Age Group: ARF primarily affects children and adolescents aged 5 to 15 years. It is rare in children under 3 years and decreases significantly in frequency after late adolescence.
- Socioeconomic Impact: Although the incidence has drastically declined in high-income countries due to routine antibiotic treatment for strep throat, it remains a massive public health crisis in low- and middle-income countries, indigenous populations, and areas with crowded living conditions.
Etiology & Risk Factors
- Primary Pathogen: Streptococcus pyogenes (Group A Beta-Hemolytic Streptococcus or GABHS). Notably, only upper respiratory tract GABHS infections (pharyngitis) trigger ARF; streptococcal skin infections (impetigo, pyoderma) do not.
- Environmental Triggers: Overcrowding, substandard housing, poverty, and limited access to healthcare drastically increase transmission rates of streptococcal pharyngitis.
- Host Susceptibility: A genetic predisposition is linked to specific human leukocyte antigen (HLA) class II types, influencing how an individual's immune system responds to streptococcal antigens.
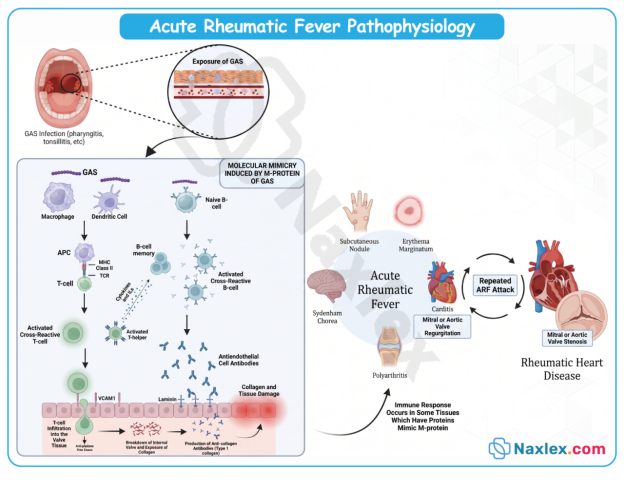
Pathophysiology
The underlying mechanism of ARF is molecular mimicry, a form of autoimmune cross-reactivity.
- Antigen Presentation: During a GABHS infection, the body creates antibodies against virulence factors on the bacterial cell wall, most notably the M-protein.
- Cross-Reactivity: The structural configuration of the streptococcal M-protein closely resembles human host proteins. The antibodies fail to distinguish between the two:
- Heart: Antibodies bind to cardiac myosin and valvular endothelium, initiating a cascade of inflammatory T-cells.
- Brain: Antibodies cross-react with lysogangliosides in the basal ganglia, disrupting dopaminergic pathways.
- Joints & Skin: Immune complexes deposit in the synovium and dermal layers, sparking acute, localized inflammation.
- Histopathology: The hallmark histological feature found in the myocardium during the acute phase is the Aschoff body, a localized area of tissue necrosis surrounded by immune cells (lymphocytes, plasma cells, and large, activated macrophages known as Anitschkow cells or "caterpillar cells").
Image Title: Acute Rheumatic Fever Pathophysiology
Clinical Manifestations
The clinical expression of ARF appears after a latent period of approximately 2 to 4 weeks following the initial strep infection. Signs are traditionally categorized into Major and Minor criteria.
Major Manifestations
- Carditis (50-70% of cases): The most serious manifestation. It presents as a pancarditis affecting the endocardium (causing valvular regurgitation, typically mitral or aortic), myocardium (causing tachycardia, cardiomegaly, or heart failure), and pericardium (causing a friction rub or chest pain).
- Migratory Polyarthritis (approx. 75% of cases): Intense inflammation affecting the large joints (knees, ankles, elbows, wrists). It is distinctively migratory, one joint becomes red, hot, swollen, and excruciatingly painful for a few days, and as it resolves, another joint becomes involved. It leaves no permanent joint damage.
- Sydenham Chorea (10-15% of cases): Also known as "St. Vitus Dance," this is a delayed CNS manifestation occurring up to several months after infection. It is characterized by sudden, involuntary, purposeless, jerky movements, accompanied by muscle weakness and emotional lability. It is more common in females and resolves completely over weeks to months.
- Erythema Marginatum (<5% of cases): A distinct, non-pruritic, erythematous rash. It features pink macules with clear centers and elevated, wavy borders, typically found on the trunk and proximal extremities. It is transient and can be accentuated by heat (e.g., a warm bath).
- Subcutaneous Nodules (<2% of cases): Small, firm, painless, mobile nodules measuring 0.5 to 2 cm. They appear in crops over bony prominences (extensor surfaces of elbows, knees, knuckles, spine) and are almost always associated with severe carditis.
Minor Manifestations
- Arthralgia: Joint pain without objective findings of inflammation (swelling, redness, warmth). Cannot be used if polyarthritis is already counted as a major criterion.
- Fever: Characteristically high-grade at the onset of acute illness (>38.5∘C or >101.3∘F).
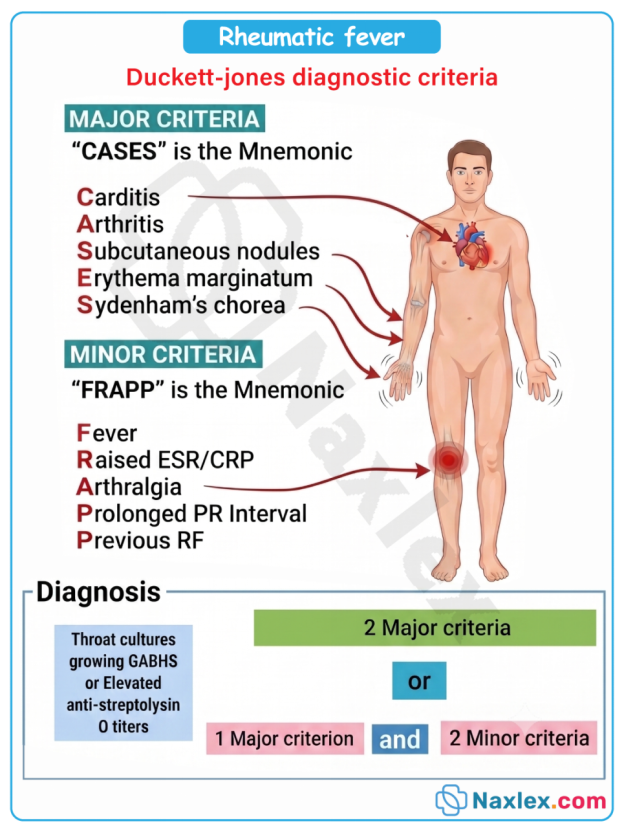
Diagnostic Evaluation
No single clinical symptom or laboratory marker is diagnostic of ARF. Clinicians rely on the Revised Jones Criteria, which requires evidence of a preceding GABHS infection PLUS either 2 major criteria OR 1 major and 2 minor criteria.
Essential Evidence of Preceding GABHS Infection
- Positive throat culture or rapid streptococcal antigen test.
- Elevated or rising streptococcal antibody titers: Anti-streptolysin O (ASO) titer (most common) or Anti-DNase B titer.
Laboratory Findings (Minor Criteria)
- Acute-Phase Reactants: Elevated Erythrocyte Sedimentation Rate (ESR) and C-Reactive Protein (CRP), reflecting systemic inflammation.
Objective Assessment Tools
- Electrocardiogram (ECG): Demonstrates a prolonged PR interval (first-degree atrioventricular block), reflecting inflammatory delay in cardiac conduction.
- Echocardiography (Echo): Essential for detecting subclinical carditis, evaluating mitral/aortic valve regurgitation, and assessing ventricular function.
Therapeutic Management
Therapeutic goals are aimed at eradicating any remaining streptococcal bacteria, controlling systemic inflammation, protecting the heart, and mitigating symptoms.
Antibiotic Therapy
- Primary Eradication: A single intramuscular injection of Penicillin G Benzathine is the treatment of choice. Alternatively, a 10-day course of oral Penicillin V or Amoxicillin is prescribed. For penicillin-allergic patients, Erythromycin, Azithromycin, or Cephalexin are used.
Anti-inflammatory Medications
- Salicylates (Aspirin): Highly effective at suppressing the joint pain and inflammation of polyarthritis.
Nursing Insight: Aspirin is used cautiously in pediatrics due to the risk of Reye's syndrome, but ARF is a specific indication where its anti-inflammatory benefits outweigh the risks under close monitoring.
- Corticosteroids (Prednisone): Reserved for patients with severe carditis or cardiomegaly to rapidly control myocardial inflammation and protect valvular function.
Supportive Therapy
- Chorea Management: For severe Sydenham chorea, anticonvulsants or sedatives such as Phenobarbital, Haloperidol, or Valproic acid may be utilized to minimize involuntary motor activity.
- Heart Failure Management: If carditis leads to heart failure, therapy includes fluid restriction, a low-sodium diet, diuretics (Furosemide), and inotropic agents (Digoxin).
Nursing Care Plan
Nursing Diagnosis 1: Decreased Cardiac Output
- Related To: Myocardial and valvular inflammation associated with acute rheumatic carditis.
- Evidenced By: Tachycardia disproportionate to fever, tachypnea, gallop rhythm, new or changing heart murmurs, orthopnea, or peripheral edema.
- Expected Outcome: The patient will maintain adequate cardiac output as evidenced by stable vital signs, clear lung fields, and strong peripheral pulses.
Nursing Interventions & Rationales
- Enforce Strict Bed Rest: Minimize metabolic demand and cardiac workload during the acute inflammatory phase. Slowly advance activity as acute-phase reactants (ESR, CRP) normalize.
- Monitor Vital Signs Continuously: Assess for resting tachycardia (a key indicator of carditis) and changes in respiratory rate or blood pressure.
- Perform Focused Cardiac Assessment: Auscultate for new murmurs (mitral regurgitation), muffled heart sounds, or a pericardial friction rub.
- Administer Prescribed Medications Safely: Give corticosteroids or diuretics as ordered; closely track intake/output and daily weights to monitor for fluid retention.
Nursing Diagnosis 2: Acute Pain
- Related To: Inflammatory immune complex deposition in the large joints (polyarthritis).
- Evidenced By: Guarding behavior, crying, reluctance to move limbs, and swollen, warm, erythematous joints.
- Expected Outcome: The patient will report a significant reduction in joint pain and display improved mobility within 24 to 48 hours of starting anti-inflammatory therapy.
Nursing Interventions & Rationales
- Administer Scheduled Salicylates (Aspirin): Provide aspirin with food or milk to minimize gastric distress; monitor closely for salicylic acid toxicity (tinnitus, tachypnea).
- Handle Joints with Extreme Gentleness: Avoid sudden movements or jerking the bed; support joints during repositioning.
- Utilize Non-Pharmacological Comfort Measures: Use bed cradles to keep heavy blankets off tender joints; apply warm compresses if tolerated.
Nursing Diagnosis 3: Risk for Injury
- Related To: Involuntary, uncoordinated motor movements associated with Sydenham chorea.
- Expected Outcome: The patient will remain free from physical trauma or injury during episodes of choreiform movements.
Nursing Interventions & Rationales
- Modify the Environment for Safety: Keep the bed in the lowest position with padded side rails up. Eliminate sharp objects from the immediate surroundings.
- Assist with Activities of Daily Living (ADLs): Provide finger foods and use unbreakable utensils to prevent injury during meals; assist with ambulation.
- Provide Emotional Support and Reassurance: Inform the child and family that these movements are temporary and will resolve completely, helping to alleviate anxiety and frustration.
Complications
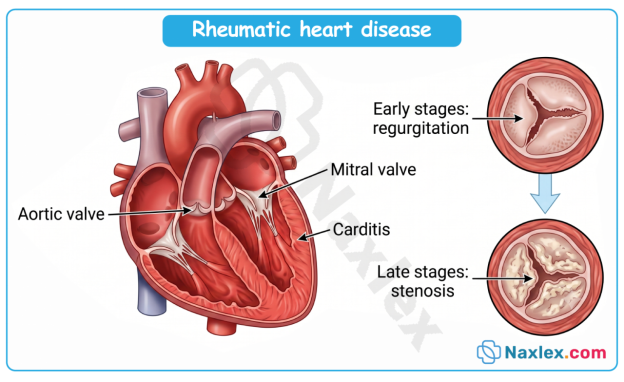
Chronic Rheumatic Heart Disease (RHD)
The most significant and devastating long-term complication of ARF. Repeated or severe bouts of rheumatic carditis lead to structural remodeling, scarring, and calcification of the cardiac valves.
- Mitral Valve Deformity: The mitral valve is the most frequently damaged structure (followed by the aortic valve). Valvular inflammation leads to mitral regurgitation in the acute phase, which can evolve over decades into mitral stenosis as the valve leaflets become rigid, thickened, and fused.
- Clinical Sequelae: RHD leads to chronic heart failure, pulmonary hypertension, and atrial fibrillation (due to left atrial enlargement from mitral stenosis), which significantly elevates stroke risk.
Other Complications
- Cardiac Arrhythmias: High-degree heart blocks or atrial tachyarrhythmias caused by conduction pathway inflammation.
Thromboembolism: Systemic emboli originating from thrombi formed in an enlarged, fibrillating left atrium.
Prognosis
The immediate prognosis of an ARF episode is generally favorable, with joint manifestations, rash, and chorea completely resolving without residual deficits. However, the overall long-term prognosis depends entirely on two primary variables:
- The Severity of the Initial Carditis: Individuals who escape the initial attack without cardiac involvement rarely develop subsequent valvular disease, provided they do not experience recurrences.
- Prevention of Recurrent Episodes: Each recurrent episode of ARF compounds previous cardiac damage. The heart becomes increasingly vulnerable with each subsequent streptococcal infection.
If recurrent infections are completely prevented through consistent antibiotic prophylaxis, even mild-to-moderate valvular damage can stabilize or improve over time.
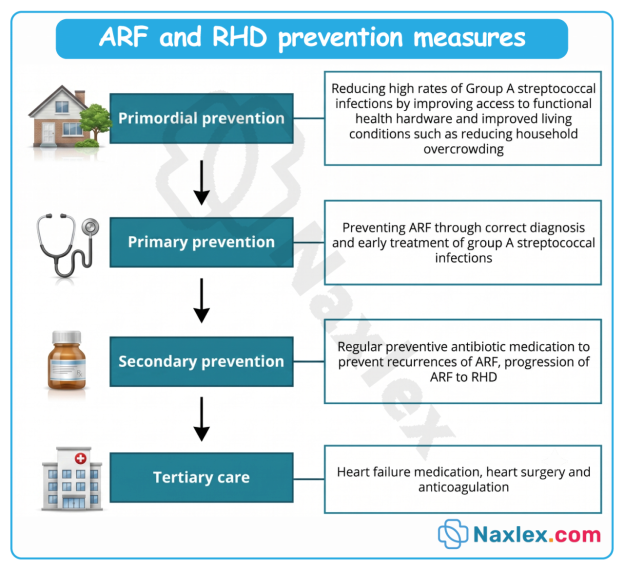
Prevention
Prevention strategies are categorized into Primary and Secondary interventions, forming the cornerstone of global rheumatic fever control.
Primary Prevention
- Goal: Prevent the initial attack of ARF.
- Intervention: Promptly diagnose and properly treat all cases of GABHS pharyngitis using a full 10-day course of oral penicillin (or an appropriate alternative) or a single injection of Benzathine Penicillin G. If antibiotic therapy is initiated within 9 days of the onset of strep throat symptoms, the risk of developing ARF is virtually eliminated.
Secondary Prevention (Long-Term Prophylaxis)
- Goal: Prevent recurrent GABHS infections that trigger recurrent episodes of ARF and worsen RHD.
- Standard Regimen: Intramuscular Penicillin G Benzathine administered every 3 to 4 weeks is the most reliable method. Oral Penicillin V or Sulfadiazine daily are alternatives but are highly dependent on patient compliance.
- Duration of Prophylaxis:
|
Patient Clinical Status |
Standard Duration of Prophylaxis |
|
ARF without Carditis |
For 5 years or until age 21 (whichever is longer) |
|
ARF with Carditis (No Residual Valve Disease) |
For 10 years or until age 21 (whichever is longer) |
|
ARF with Carditis + Residual Valvular Disease |
For 10 years or until age 40 (whichever is longer); sometimes lifelong |