
Ati Maternal Newborn 4 Proctored Exam
Ati Maternal Newborn 4 Proctored Exam
Total Questions : 49
Showing 10 questions Sign up for moreA nurse suspects that a pregnant client may be experiencing placenta abruption based on assessment of which finding? Select all that apply.
Explanation
Choice A: Absence of pain is not a sign of abruptio placenta. Abruptio placenta is a condition where the placenta separates from the uterine wall before delivery, causing bleeding and pain. The pain is usually severe and constant.
Choice B: Insidious onset is not a sign of abruptio placenta. Abruptio placenta is usually a sudden and acute event that occurs in the third trimester or during labor.
Choice C: Dark red vaginal bleeding is a sign of abruptio placenta. The bleeding is caused by the rupture of blood vessels between the placenta and the uterus. The blood may be dark red because it is old or clotted.
Choice D: Rigid uterus is a sign of abruptio placenta. The uterus becomes hard and tense as a result of the bleeding and contraction of the uterine muscles. This can impair the blood flow to the fetus and cause fetal distress.
Choice E: Absent fetal heart tones is a sign of abruptio placenta. The loss of blood and oxygen to the fetus can cause fetal death or stillbirth. Fetal heart tones can be detected by using a Doppler device or a fetoscope.

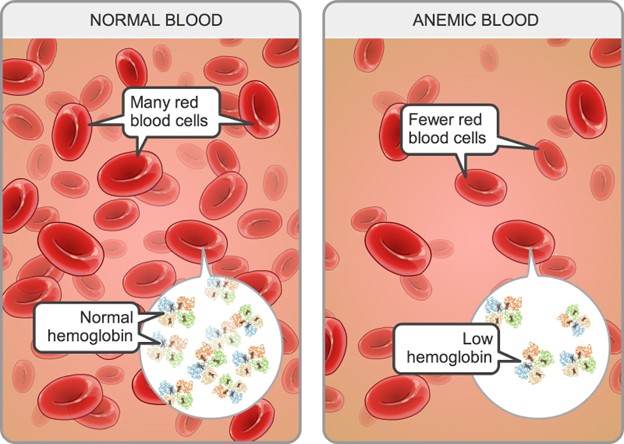
A pregnant client in her second trimester has a hemoglobin level of 11 g/dL. The nurse interprets this as indicating
Explanation
Choice A: Hemodilution of pregnancy is a normal physiological phenomenon that occurs when the plasma volume increases more than the red blood cell mass, resulting in a lower hemoglobin concentration. The normal hemoglobin range for pregnant women in the second trimester is 10.5 to 14 g/dL.
Choice B: A multiple gestation pregnancy may cause a higher hemoglobin level due to increased erythropoietin production by the placenta. The normal hemoglobin range for pregnant women with twins in the second trimester is 12 to 16 g/dL.
Choice C: Greater-than-expected weight gain is not related to hemoglobin level. Weight gain during pregnancy depends on various factors such as pre-pregnancy weight, nutrition, activity level, and fetal growth.
Choice D: Iron-deficiency anemia is a condition where the hemoglobin level is below the normal range due to inadequate iron intake or absorption, blood loss, or increased iron demand. The signs and symptoms of iron-deficiency anemia include fatigue, pallor, weakness, shortness of breath, and pica.
A pregnant client in her second trimester has a hemoglobin level of 11 g/dL. The nurse interprets this as indicating
Explanation
Choice A: Hemodilution of pregnancy is a normal physiological phenomenon that occurs when the plasma volume increases more than the red blood cell mass, resulting in a lower hemoglobin concentration. The normal hemoglobin range for pregnant women in the second trimester is 10.5 to 14 g/dL.
Choice B: A multiple gestation pregnancy may cause a higher hemoglobin level due to increased erythropoietin production by the placenta. The normal hemoglobin range for pregnant women with twins in the second trimester is 12 to 16 g/dL.
Choice C: Greater-than-expected weight gain is not related to hemoglobin level. Weight gain during pregnancy depends on various factors such as pre-pregnancy weight, nutrition, activity level, and fetal growth.
Choice D: Iron-deficiency anemia is a condition where the hemoglobin level is below the normal range due to inadequate iron intake or absorption, blood loss, or increased iron demand. The signs and symptoms of iron-deficiency anemia include fatigue, pallor, weakness, shortness of breath, and pica.
A nurse is providing prenatal care to a pregnant client. At which time would the nurse expect to screen the client for group B streptococcus infection?
Explanation
Choice A: 28 weeks' gestation is too early to screen for group B streptococcus infection. Group B streptococcus (GBS) is a type of bacteria that can cause serious infections in newborns if transmitted from the mother during labor and delivery. The optimal time to screen for GBS is between 35 and 37 weeks' gestation.
Choice B: 32 weeks' gestation is also too early to screen for GBS infection. Screening at this time may not reflect the true colonization status of the mother at the time of delivery, as GBS can be transient or intermittent.
Choice C: 16 weeks' gestation is much too early to screen for GBS infection. Screening at this time has no clinical value, as GBS colonization can change throughout pregnancy.
Choice D: 36 weeks' gestation is the appropriate time to screen for GBS infection. Screening at this time can identify mothers who are colonized with GBS and who need intrapartum antibiotic prophylaxis to prevent neonatal sepsis, pneumonia, and meningitis.
A nurse is providing teaching about nutrition to a client at her first prenatal visit. Which of the following statements by the nurse should be included in the teaching?
Explanation
Choice A: Vitamin E requirements do not decrease during pregnancy due to the increase in body fat. Vitamin E is a fat-soluble vitamin that acts as an antioxidant and protects cell membranes from oxidative damage. The recommended dietary allowance (RDA) for vitamin E during pregnancy is 15 mg/day, which is the same as for non-pregnant women.
Choice B: Prenatal vitamins will meet your need for increased folic acid during pregnancy. Folic acid is a water-soluble vitamin that is essential for DNA synthesis and cell division. Folic acid deficiency can cause neural tube defects in the fetus, such as spina bifida and anencephaly. The RDA for folic acid during pregnancy is 600 mcg/day, which can be obtained from prenatal vitamins and fortified foods.
Choice C: You will not need to double your intake of protein during pregnancy. Protein is a macronutrient that provides amino acids for tissue growth and repair. The RDA for protein during pregnancy is 1.1 g/kg/day, which is only slightly higher than for non-pregnant women (0.8 g/kg/day).
Choice D: You will not need to increase your intake of calcium during pregnancy. Calcium is a mineral that is important for bone health and muscle contraction. Calcium absorption and retention are enhanced during pregnancy, so there is no need to increase the intake above the RDA of 1000 mg/day for women aged 19 to 50 years.
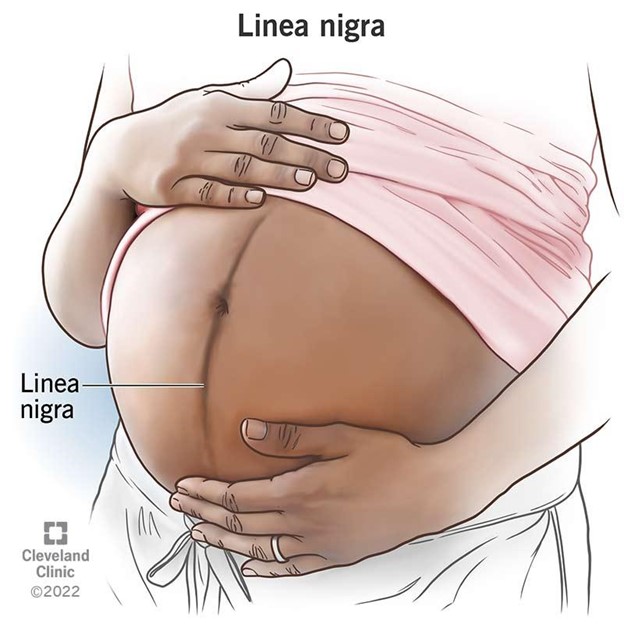
Assessment of a pregnant woman reveals a pigmented line down the middle of her abdomen. The nurse documents this as which finding?
Explanation
Choice A: Striae gravidarum are stretch marks that appear on the abdomen, breasts, or thighs during pregnancy. They are caused by the tearing of the connective tissue in the dermis due to rapid growth or weight gain.
Choice B: Linea nigra is a dark vertical line that runs from the umbilicus to the pubic area. It is caused by increased melanin production due to hormonal changes during pregnancy. This is the correct choice because it matches the description in the question.
Choice C: Vascular spiders are dilated blood vessels that appear on the skin as red or purple spider-like lesions. They are caused by increased estrogen levels and blood volume during pregnancy. They are usually found on the face, neck, chest, or arms.
Choice D: Melasma is a condition that causes brown or gray patches on the face, especially on the forehead, cheeks, nose, or upper lip. It is caused by increased melanin production due to sun exposure and hormonal changes during pregnancy. It is also known as chloasma or the mask of pregnancy.
A client with hyperemesis gravidarum is admitted to the facility after being cared for at home without success. What would the nurse expect to include in the client's plan of care?
Explanation
Choice A: A clear liquid diet is not appropriate for a client with hyperemesis gravidarum, which is a severe form of nausea and vomiting during pregnancy that can lead to dehydration, electrolyte imbalance, and weight loss. A clear liquid diet does not provide adequate calories, protein, vitamins, or minerals for the client and the fetus.
Choice B: Administration of diethylstilbestrol is not indicated for a client with hyperemesis gravidarum. Diethylstilbestrol is a synthetic estrogen that was used in the past to prevent miscarriage and premature birth, but it was found to cause serious adverse effects such as vaginal cancer, infertility, and birth defects in the offspring.
Choice C: Total parenteral nutrition is the correct choice because it provides a complete and balanced source of nutrients through a central venous catheter. It is used for clients who cannot tolerate oral or enteral feeding due to severe gastrointestinal disorders such as hyperemesis gravidarum. It helps to prevent malnutrition, dehydration, and ketosis in the client and the fetus.
Choice D: Nothing by mouth is not a suitable option for a client with hyperemesis gravidarum. It can worsen the condition by causing starvation, acidosis, and ketosis. It can also increase the risk of aspiration pneumonia if the client vomits.
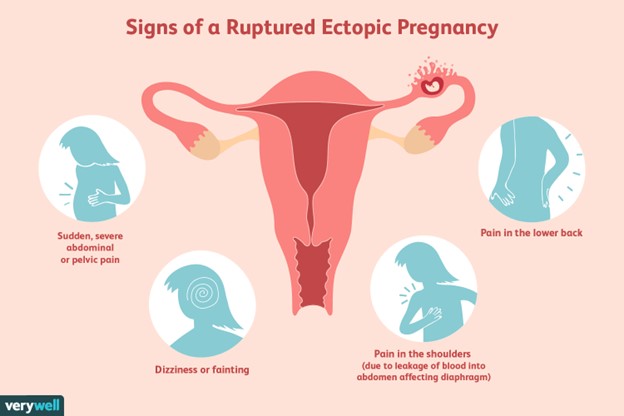
A client is suspected of having a ruptured ectopic pregnancy. Which assessment would the nurse identify as the priority?
Explanation
Choice A reason: Hemorrhage is the most life-threatening complication of a ruptured ectopic pregnancy, as it can lead to hypovolemic shock and death. The nurse should monitor the client's vital signs, blood loss, and level of consciousness, and administer fluids and blood products as ordered.
Choice B reason: Edema is not a common sign of a ruptured ectopic pregnancy, and it is not a priority over hemorrhage. Edema may be caused by other conditions, such as heart failure, kidney disease, or venous insufficiency.
Choice C reason: Infection is a possible complication of a ruptured ectopic pregnancy, but it is not as urgent as hemorrhage. Infection may manifest as fever, chills, malaise, or foul-smelling vaginal discharge. The nurse should administer antibiotics as ordered and monitor the client's temperature and white blood cell count.
Choice D reason: Jaundice is not a typical symptom of a ruptured ectopic pregnancy, and it is not a priority over hemorrhage. Jaundice may indicate liver dysfunction or hemolytic anemia, which are unrelated to ectopic pregnancy. The nurse should assess the client's skin and sclera color, and check the liver enzymes and bilirubin levels.
Upon entering the room of a client who has had a spontaneous abortion, the nurse observes the client crying. Which response by the nurse would be most appropriate?
Explanation
Choice A Reason: This is the correct answer because it is an empathetic and supportive response that acknowledges the client's loss and grief. This is an empathetic and supportive response that acknowledges the client's loss and grief. The other choices are inappropriate because they are insensitive, dismissive, or inaccurate.
Choice B Reason: This is an inappropriate answer because it implies that the nurse does not understand or care about the client's emotional state. It also suggests that the client has no Reason to cry, which is invalidating and hurtful.
Choice C Reason: This is an inappropriate answer because it focuses on the physical pain rather than the emotional pain of the client. It also implies that the nurse wants to avoid dealing with the client's feelings and just give them a medication to make them stop crying.
Choice D Reason: This is an inappropriate answer because it is inaccurate and misleading. A spontaneous abortion, also known as a miscarriage, occurs when a pregnancy ends before 20 weeks of gestation. At this stage, the baby is already formed and has a heartbeat, organs, and limbs. Saying that a baby still wasn't formed in the womb is false and insensitive to the client's loss.
Assessment of a pregnant woman reveals that she compulsively craves ice. The nurse documents this finding as
Explanation
Choice A Reason: Linea nigra is a dark vertical line that appears on the abdomen of some pregnant women. It is caused by increased melanin production and usually fades after delivery.
Choice B Reason: Pica is a condition in which a person has an abnormal desire to eat substances that are not food, such as ice, clay, dirt, or chalk. It is more common in pregnant women and may indicate a deficiency in iron or other nutrients.
Choice C Reason: Ballottement is a technique of palpating a floating structure by bouncing it gently and feeling it rebound. In obstetrics, it can be used to detect the presence of the fetus by feeling its head move when the cervix is tapped.
Choice D Reason: Quickening is the first perception of fetal movements by the pregnant woman. It usually occurs between 16 and 20 weeks of gestation.
You just viewed 10 questions out of the 49 questions on the Ati Maternal Newborn 4 Proctored Exam Exam. Subscribe to our Premium Package to obtain access on all the questions and have unlimited access on all Exams. Subscribe Now

