
Please set your exam date
Acquired Cardiovascular Disorders: Infective Endocarditis
Study Questions
Practice Excercise 3
The nurse is assessing a child admitted with left-sided infective endocarditis. Which clinical findings would indicate systemic embolic complications resulting from vegetations on this side of the heart? Select all that apply
Explanation
Left-sided infective endocarditis vegetationspose a severe threat of systemic arterial fragmentation. When fragments dislodge from the mitral or aortic valves, they enter the systemic arterial circulation, leading to cerebrovascular ischemia, renal infarction,or acute limb occlusiondepending on the final vascular bed where the emboli lodge.
Rationale for correct answers:
1.A cerebrovascular accidentmanifests as sudden hemiparesis and facial droopingwhen septic emboli travel up the carotid arteries into the cerebral circulation. This occludes middle or anterior cerebral vessels, causing acute ischemic tissue necrosis.
2.The renal infarctionpresents clinically with acute flank pain and macrovascular hematuria. Septic fragments traveling down the descending aorta divert into the renal arteries, wedging within the parenchymal microvasculature and causing focal tissue necrosis.
3.An acute limb ischemiatriggers the classic clinical findings of pain, pallor, and pulselessnessin the extremity. This occurs when an arterial embolus migrates distally into the femoral or popliteal segments, terminating peripheral perfusion.
Rationale for incorrect answers:
4.The pleuritic chest painaccompanied by dyspneais characteristic of septic pulmonary emboli,which occur in right-sided infective endocarditis. Left-sided emboli travel out to the systemic arterial tree rather than entering the pulmonary arterial vasculature.
5.The bilateral crackleswith a clear radiographdo not indicate a systemic embolic phenomenon. While left-sided valvular failure can cause pulmonary congestion, crackles represent fluid shifts or alveolar dysfunction rather than direct systemic arterial embolic migration.
Test-taking strategy:
- Analyze the scenario/question: The nurse is assessing a child with left-sided infective endocarditis. The question requires selecting all clinical findings that indicate systemic embolic complications arising from this specific side of the heart.
- Apply vascular anatomy:
- Left-sided cardiac structures pump blood directly into the systemic arterial circulation, meaning emboli will travel to the brain, viscera, and extremities.
- Rule in Choice 1because cerebral arterial occlusion causes sudden neurological deficits like hemiparesis.
- Rule in Choice 2because renal arterial occlusion presents with localized flank pain and hematuria.
- Rule in Choice 3because peripheral arterial occlusion leads to signs of acute limb ischemia.
- Eliminate right-sided and non-embolic signs:
- Rule out Choice 4because pulmonary embolic signs are a consequence of right-sided vegetations migrating to the lungs.
- Rule out Choice 5because adventitious breath sounds reflect fluid overload or heart failure dynamics rather than systemic arterial embolism.
Take home points
- Left-sided infective endocarditis carries a high risk of systemic embolic events affecting the brain, kidneys, spleen, and extremities.
- Right-sided infective endocarditis typically causes pulmonary embolic complications due to the direction of right ventricular output.
- Sudden neurological changes in a patient with left-sided vegetations warrant immediate emergency imaging to rule out a stroke.
- Acute abdominal or flank pain in these patients frequently points to splenic or renal microvascular infarction.
A 10-year-old child with a history of congenital aortic stenosis is admitted with a suspected diagnosis of subacute infective endocarditis. Which order should the nurse execute first?
Explanation
Subacute infective endocarditisinvolves microbial colonization of damaged valvular endothelium, commonly caused by Viridans streptococci.This leads to platelet-fibrin deposition,creating friable vegetations. Clinical manifestations include low-grade fever, splinter hemorrhages, Roth spots, and a new or changing cardiac murmur.
Rationale for correct answer
2.Obtaining blood cultures before administering antibioticsis the absolute priority to avoid suppressing microbial growth.Culturing ensures precise pathogen identification and targeted antimicrobial therapy. Isolating the causative agent prevents false-negative results and guides long-term bactericidal treatmentparameters. Three distinct venipuncture sites maximize diagnostic sensitivity and exclude potential sample contamination.
Rationale for incorrect answers
1.Administering broad-spectrum antibiotics prior to obtaining blood culturesis strictly contraindicated in stable patients. Doing so can sterilize the bloodstream rapidly, masking the true causative pathogen.Delayed or inaccurate pathogen identification can lead to inappropriate long-term empiric therapy choices. Antibiotic initiation must immediately follow the completion of the culture collection process.
3.A baseline chest X-rayprovides valuable structural data but is not a time-critical intervention. It helps evaluate pulmonary congestion or cardiomegalyassociated with valvular dysfunction. However, radiographic imaging does not directly guide the critical antimicrobial management required for endocarditis. It must be deferred until after blood cultures are successfully drawn.
4.An echocardiogramis essential for visualizing valvular vegetationsand assessing overall cardiac function.While vital for confirming the diagnosis, scheduling it for the next morning is acceptable. It does not take precedence over immediate diagnostic sequencing needs in the emergency department. The delay does not compromise immediate stabilizing interventions or culture collection.
Test-taking strategy:
- Analyze the scenario/question: A 10-year-old patient with congenital aortic stenosis has suspected subacute infective endocarditis. The nurse must determine which clinical intervention requires immediate, first-priority execution.
- Apply prioritization principles:
- In cases of suspected systemic infections, diagnostic identification must always precede therapeutic neutralization.
- Administering medications before culturing destroys diagnostic accuracy, violating core safety and nursing care standards.
- Evaluate choices:
- Rule inChoice 2:Drawing blood culturesis the mandatory first step to isolate the pathogen before any antibiotics alter the intravascular environment.
- Rule outChoice 1:Giving IV Ampicillinmust be delayed until cultures are drawn to avoid false-negative diagnostic panels.
- Rule outChoice 3:A chest X-rayis a secondary diagnostic tool for structural assessment and is never prioritized over sepsis protocols.
- Rule outChoice 4: An echocardiogramconfirms vegetative growth but can be safely scheduled after initial laboratory work is secured.
Take home points
- Blood cultures must always be obtained prior to the administration of the first dose of antibiotics to prevent false-negative results.
- Subacute infective endocarditis typically presents insidiously in patients with pre-existing congenital heart defects like aortic stenosis.
- A minimum of three separate blood culture samples drawn from different sites is necessary to accurately diagnose bloodborne pathogens.
- Echocardiography is the gold standard imaging modality used to visualize valvular vegetations and assess myocardial complications.
A pediatric nurse is preparing discharge education for the parents of a 5-year-old child who survived an episode of S. aureus endocarditis and has a normal native mitral valve. Which statement by the parents indicates an accurate understanding of the prevention guidelines?
Explanation
Infective endocarditis prophylaxis avoids endocardial endothelial damageduring invasive procedures. High-risk cohorts encompass previous endocarditis and unrepaired cyanotic congenital heart defects.Transient bacterial inoculationcan trigger dangerous endovascular microbial colonization.
Rationale for correct answer:
1.A previous history of endocarditis requires lifelong antimicrobial prophylaxisbefore invasive dental interventions.This mandate persists even if native valves escaped structural damage during infection. Pre-procedural amoxicillin neutralizes oral floraintroduced into systemic circulation. This standard effectively mitigatesrecurrent endothelial colonizationover the lifespan.
Rationale for incorrect answers:
2.Restricting antibiotic prophylaxis to a 6-month healing windowrepresents an erroneous interpretation of pediatric preventive guidelines. Endothelial vulnerability remains permanently elevated following any initial endocardial infection. Endocarditis history alters the endovascular substrate, leaving it susceptible to future pathogen adherence. Consequently, prophylactic protocolscannot be discontinued after a temporary convalescence period.
3.Assuming structurally intact native valves eliminate the necessity for dental antibiotic premedicationis clinically incorrect. The American Academy of Pediatrics specifies a history of endocarditis as an independent high-risk stratificationcriterion. Endothelial surfaces possess microscopic changes that facilitate subsequent bacterial attachment despite normal gross morphology. Therefore, prophylactic amoxicillinremains mandatory for all subsequent tissue-manipulating dental care.
4.Administering a daily maintenance antibiotic pillis an inappropriate strategy for long-term endocarditis prevention. Continuous daily therapy breeds antimicrobial resistanceand alters the host microbiome without providing targeted procedural protection. Prophylaxis is strictly indicated as a single pre-procedural dose rather than continuous suppressive therapyregimens. This targeted approach balances effective infection prevention with sound antimicrobial stewardship.
Test-taking strategy:
- Analyze the scenario/question: A 5-year-old child survived S. aureusendocarditis and has a normal native mitral valve. The nurse must identify the correct parental statement regarding long-term infective endocarditis prevention.
- Apply prophylaxis guidelines:
- Previous history of infective endocarditis places a patient into the highest risk category for adverse outcomes.
- High-risk patients require lifelong subacute bacterial endocarditis prophylaxis for dental procedures involving gingival manipulation.
- Evaluate choices:
- Rule inChoice 1:The parents correctly state that oral antibioticsare required before every routine dental cleaning for life due to the past endocarditis history.
- Rule outChoice 2:Antibiotic coverage is not limited to a short 6-monthpostoperative or recovery timeline.
- Rule outChoice 3:Having a normal native valve does not remove the absolute need for prophylactic coveragegiven the prior history.
- Rule outChoice 4:Daily administration of maintenance medication represents chronic suppressionrather than targeted procedural prophylaxis.
Take home points
- Blood cultures must always be obtained prior to the administration of the first dose of antibiotics to prevent false-negative results.
- Subacute infective endocarditis typically presents insidiously in patients with pre-existing congenital heart defects like aortic stenosis.
- A minimum of three separate blood culture samples drawn from different sites is necessary to accurately diagnose bloodborne pathogens.
- Echocardiography is the gold standard imaging modality used to visualize valvular vegetations and assess myocardial complications.
A 12-year-old child with a mechanical mitral valve replacement is scheduled for a routine dental cleaning. The provider orders Amoxicillin prophylaxis. What is the correct protocol for the nurse to verify?
Explanation
Infective endocarditis prophylaxisprevents bacterial endocardial colonizationduring invasive dental procedures. High-risk substrates include prosthetic cardiac valvesand previous endocarditis episodes. Transient bacteremia from gingival tissue manipulationcan precipitate devastating valvular endothelial infection.
Rationale for correct answer:
2.Administering amoxicillin 30 to 60 minutes prior to proceduresensures peak serum concentrations during transient bacteremia.High circulating levels block oral pathogens from adhering to the prosthetic valve matrix. This timing optimizesbactericidal drug efficacyduring tissue manipulation. It provides maximal protection against endocardial inoculation.
Rationale for incorrect answers:
1.Administering the medication 2 hours after dental workfinishes fails to provide proactive endocardial protection. Post-procedural delivery allows circulating bacteria to colonize the mechanical hardware before therapeutic serum concentrationsare achieved. Late administration cannot dislodge pathogens that have already adhered to fibrin-platelet thrombi.This timing renders the prophylaxis clinically ineffective.
3.Prescribing amoxicillin every 8 hours for 3 days leading up to the appointmentis incorrect. This prolonged regimen does not improve procedural protection and promotes antimicrobial resistance selectionwithin oral flora. It unnecessarily alters the patient's microbiome without providing additional bactericidal peak utilityduring tissue manipulation. Standard protocols strictly mandate a single pre-procedural dose.
4.Canceling routine dental cleanings because mechanical hardwareis present is a severe clinical error. Maintaining excellent oral health through professional scaling reduces the overall baseline incidence of spontaneous bacteremia episodes.Professional care is entirely safe when executed with appropriate pre-procedural antibiotic coverage.Denying routine hygiene increases long-term periodontal risk.
Test-taking strategy:
- Analyze the scenario/question: A 12-year-old child with a mechanical mitral valve replacement requires a routine dental cleaning. The nurse must verify the correct administrative protocol for prophylactic Amoxicillin.
- Apply Prophylaxis Standards:
- Prophylactic antibiotics must be present in the bloodstream at peak concentrations at the exact time tissue damage and bacterial inoculation happen.
- Standard guidelines from major cardiac societies designate a strict timeline of 30 to 60 minutes prior to procedural initiation.
- Evaluate Choices:
- Rule inChoice 2:Giving the drug 30 to 60 minutes before the procedure maximizes serum concentrationsduring the period of peak bacterial entry.
- Rule outChoice 1:Post-procedural administration at 2 hoursallows bacteria to bind to the mechanical hardware without any antimicrobial interference.
- Rule outChoice 3:A 3-day courseis completely unnecessary, increases adverse side effects, and accelerates the development of bacterial resistance patterns.
- Rule outChoice 4:Dental scaling is never contraindicatedfor these children, provided they receive the proper prophylactic medication regimen beforehand.
Take home points
- Prophylactic amoxicillin must be administered 30 to 60 minutes before dental procedures to ensure peak serum levels during tissue manipulation.
- Mechanical heart valve replacements place pediatric patients in the highest risk category for developing infective endocarditis from transient bacteremia.
- Routine dental hygiene is critical for high-risk patients because chronic oral infections significantly increase the risk of spontaneous bacteremia.
- Prophylaxis guidelines require a single pre-procedural dose rather than multi-day antibiotic regimens to limit antimicrobial resistance.
The nurse is caring for a group of pediatric clients. Which of the following scenarios describes a patient who requires mandatory antibiotic prophylaxis prior to a dental extraction?
Explanation
Infective endocarditis prophylaxis targets specific high-risk structural substratesvulnerable to bacteremia during invasive dental procedures. High-risk categories encompass previous endocarditis episodes, prosthetic heart valves, and unrepaired or partially repaired cyanotic congenital defects.Tissue manipulation can introduce oral commensals, inducing endovascular microbial colonization.
Rationale for correct answer:
3.Repaired Tetralogy of Fallot accompanied by a residual shunt next to a prosthetic patchrepresents a critical risk factor. The presence of residual hemodynamic turbulence near synthetic patch materialhinders proper endothelialization. This creates an ideal substrate for bacterial adherence during transient procedural bacteremia. Therefore, lifelong pre-procedural antibiotic administration remains mandatory for this specific category of complex congenital defects.
Rationale for incorrect answers:
1.A ventricular septal defect that has been fully repaired without any residual shuntdoes not require antibiotic prophylaxis after 6 months. Endothelialization of the surgical site finishes well before the 2-year post-operative mark. Without turbulent blood flow or exposed synthetic material, the patient's risk of developing endocardial infection mirrors the general population. Consequently, continuous prophylactic antibiotic managementis clinically unnecessary for routine dental extractions.
2.Mild, isolated pulmonic stenosisis categorized as a low-risk cardiac anomaly according to modern pediatric guidelines. The American Heart Association explicitly excludes simple acyanotic valvular lesions from pre-procedural prophylactic requirements. The low hemodynamic pressure gradient across the pulmonic valve minimizes the likelihood of endocardial endothelial damage. Subjecting this child to antibiotics would provide no clinical benefit while increasing the risk of microbiome disruption.
4.A functional secundum atrial septal defectinvolves low-pressure left-to-right shunting that rarely causes endothelial erosion. Simple atrial defects do not predispose the endocardium to bacterial colonization during routine bacteremic events. Current clinical evidence supports omitting prophylactic antimicrobial coverfor all isolated secundum defects during invasive oral surgery. Forcing antibiotic use in this patient violates standard antimicrobial stewardship principles.
Test-taking strategy:
- Analyze the scenario/question: The nurse must identify which pediatric patient requires mandatory antibiotic prophylaxis prior to an invasive dental extraction.
- Apply risk stratification guidelines:
- Prophylaxis is restricted to patients with the highest risk of adverse outcomes from infective endocarditis, including prosthetic material with residual defects.
- Completely repaired defects without shunts after 6 months, simple acyanotic stenosis, and isolated atrial septal defects do not qualify for prophylaxis.
- Evaluate choices:
- Rule inChoice 3:A child with repaired Tetralogy of Fallot and a residual shunt near a synthetic patchhas a permanent high-risk mandate due to endothelial turbulence.
- Rule outChoice 1:A fully repaired VSD at 2 yearspost-op requires no prophylaxis because the surgical site has completely endothelialized.
- Rule outChoice 2:Mild pulmonic stenosis is an acyanotic lesion that does not create the structural vulnerability needed to justify prophylactic intervention.
- Rule outChoice 4:An isolated secundum ASD does not cause severe shear stress, meaning pre-procedural antibioticsare completely unnecessary.
Take home points
- Antibiotic prophylaxis is mandatory for dental procedures in patients with repaired congenital heart defects that leave a residual shunt adjacent to prosthetic material.
- Congenital heart defects that are fully repaired using synthetic patches only require antibiotic prophylaxis for the first 6 months following the surgical procedure.
- Acyanotic cardiac lesions, including isolated atrial septal defects and mild pulmonic stenosis, do not require pre-procedural antibiotic prophylaxis.
- The primary goal of risk stratification in endocarditis guidelines is to protect ultra-high-risk endocardial surfaces while avoiding unnecessary widespread antibiotic overuse.
The nurse is planning educational sessions for a child with a corrected ventricular septal defect who still requires infective endocarditis prophylaxis. The nurse instructs the parents that prophylaxis is indicated for which upcoming procedure?
Explanation
Infective endocarditis prophylaxis targets invasive procedures that induce significant transient bacteremiavia specific mucosal surfaces. High-risk anatomical zones include the oral cavity architectureand upper respiratory tract. Procedural trauma allows commensal microflora to breach barriers, causing dangerous endovascular bacterial dissemination.
Rationale for correct answer:
3.Dental extractions involving manipulation of gingival tissuecause significant bacteremia, introducing virulent strains into the bloodstream. These microbes can adhere to vulnerable endocardial surfaces, especially around complex congenital septal defects.Pre-procedural amoxicillin creates bactericidal serum levels that effectively neutralize these circulating pathogens. This targeted prevention minimizes the risk of secondary endocardial colonization.
Rationale for incorrect answers:
1.Routine high-wire orthodontic adjustments do not require antibiotic prophylaxisbecause they do not involve significant mucosal trauma. While appliances exert localized pressure to shift teeth, they do not disrupt the protective gingival barrier. Current pediatric guidelines explicitly exclude routine orthodontic manipulation from prophylactic antibiotic regimens.Unnecessary antibiotic administration in this scenario introduces risks without offering any measurable clinical benefit for endovascular risk mitigation.
2.Insertion of tympanostomy pressure-equalizing tubesdoes not require infective endocarditis prophylaxis under current clinical guidelines. The American Heart Association explicitly excludes clean, non-infected ear, nose, and throat surgeries from routine pre-procedural antibiotic mandates. The specific microbial flora of the middle ear rarely precipitates subacute bacterial endocarditis.Consequently, implementing prophylaxis for this procedure violates standard antimicrobial stewardship protocols.
4.Diagnostic upper gastrointestinal endoscopydoes not warrant routine antibiotic prophylaxis for endocarditis prevention. Modern clinical evidence indicates that diagnostic upper gastrointestinal procedures carry an extremely low risk of inducing significant bacteremia. Routine prophylaxis is no longer recommended for gastrointestinal or genitourinary interventions unless an active, deep-tissue infection is present. Restricting antibiotic use prevents unnecessary complications like clostridioides difficile overgrowth.
Test-taking strategy:
- Analyze the scenario/question: A child with a corrected ventricular septal defect who requires infective endocarditis prophylaxis is undergoing an upcoming procedure. The nurse must identify the specific procedure that requires mandatory pre-procedural antibiotic administration.
- Apply procedure selection guidelines:
- Infective endocarditis prophylaxis is strictly limited to dental procedures that involve significant manipulation of gingival tissue, the periapical region of teeth, or perforation of the oral mucosa.
- Routine gastrointestinal, genitourinary, and clean respiratory or otolaryngologic procedures are excluded from standard prophylaxis guidelines.
- Evaluate choices:
- Rule inChoice 3:A dental extraction requires mandatory prophylaxisbecause manipulating the gingival tissue introduces oral streptococci directly into the venous circulation.
- Rule outChoice 1:Orthodontic adjustments do not breach the deep mucosal or gingival boundaries, making pre-procedural amoxicillinunnecessary.
- Rule outChoice 2:Inserting tympanostomy tubesis a clean middle-ear procedure that does not involve the specific high-risk bacteremic pathways associated with endocarditis.
- Rule outChoice 4:An upper endoscopyis a diagnostic mucosal visualization that carries a negligible bacteremic risk, eliminating the need for routine antibiotic coverage.
Take home points
- Antibiotic prophylaxis is required for high-risk cardiac patients undergoing dental procedures that manipulate gingival tissue or perforate oral mucosa.
- Routine orthodontic appliance adjustments and the placement of high-wire braces do not require pre-procedural infective endocarditis prophylaxis.
- Clean otolaryngologic surgeries, such as the insertion of tympanostomy pressure-equalizing tubes, are excluded from routine endocarditis prophylaxis guidelines.
- Gastrointestinal diagnostic interventions, including upper endoscopies and colonoscopies, do not warrant prophylactic antibiotic administration for endocarditis prevention.
The nurse is evaluating an adolescent client with a history of infective endocarditis. The client asks why meticulous dental hygiene is emphasized so strongly. The nurse explains that proper oral care prevents:
Explanation
Meticulous dental hygieneminimizes spontaneous bacteremia episodesarising from routine daily activities like mastication and brushing. Chronic periodontal inflammation compromises the oral mucosal barrier, facilitating steady microbial translocation. Eliminating local inflammation protects the endovascular endothelial surfacefrom continuous pathogen exposure.
Rationale for correct answer:
3.Maintaining rigorous oral hygiene prevents microscopic breaches in the gingival tissuethat serve as entry portals for pathogens. Regular brushing and flossingeliminate the bacterial plaques that cause chronic local inflammation and tissue friability. A healthy, intact mucosal barrier blocks oral streptococci from accessing the systemic venous circulation.This continuous defense directly reduces the incidence of spontaneous endocardial seeding.
Rationale for incorrect answers:
1.Proper oral hygiene does not serve to prevent the overgrowth of fungal organismswithin the stomach. Gastric acidity maintains an hostile environment that naturally regulates microflora populations in the lower gastrointestinal tract. Poor oral health primarily increases the risk of local bacterial multiplication rather than systemic mycotic proliferation.There is no physiological link between daily tooth flossing and gastric fungal colonization.
2.Localized gingival inflammation does not carry a risk of transforming into a malignant oral tumor.Chronic periodontitis can lead to alveolar bone destruction, tooth loss, and severe local tissue recession if left untreated. However, the underlying pathology remains strictly inflammatory and infectious rather than neoplastic cellular transformation.Counseling must focus on realistic infectious risks rather than oncological progression warnings.
4.Oral saliva enzymes do not possess the biochemical capacity to degrade cardiac prosthetic materials.Synthetic components like titanium, Dacron, and mechanical valves are engineered to withstand physiologic shear stress and chemical exposure. Salivary enzymes remain localized within the upper digestive tract and do not circulate in the bloodstream to cause prosthetic hardware breakdown.Valvular destruction occurs through microbial enzymatic digestion during an active endovascular infectious process.
Test-taking strategy:
- Analyze the scenario/question: An adolescent client with a history of infective endocarditis asks about the physiological rationale behind the strong emphasis on meticulous dental hygiene.
- Correlate pathology with hygiene:
- Daily activities like chewing and brushing cause more frequent, cumulative bacteremia in patients with poor oral health than isolated dental procedures.
- Keeping the gums healthy reduces tissue friability, preserving the physical barrier that prevents bacteria from entering the bloodstream.
- Evaluate choices:
- Rule inChoice 3:Excellent oral care keeps the oral mucosaintact, stopping bacteria from crossing into the vascular system during everyday life.
- Rule outChoice 1:Gastric environment control is managed by stomach acidproduction, not by the frequency of mechanical tooth brushing.
- Rule outChoice 2:Chronic gingivitis results in tissue degradation and tooth loss, but does not induce malignant neoplasiain the oral cavity.
- Rule outChoice 4:Mechanical valves are completely immune to salivary enzymes,which never enter the intravascular space in active forms.
Take home points
- Meticulous daily oral hygiene is the most effective way to minimize the risk of spontaneous bacteremia from routine activities like chewing.
- Chronic gingival inflammation breaks down the mucosal barrier, allowing oral bacteria easy access to the systemic bloodstream.
- Frequent low-grade bacteremia from poor oral health poses a greater cumulative endocarditis risk than an isolated dental cleaning procedure.
- Cardiovascular prosthetic materials are structurally degraded by bacterial vegetations and immune complexes, never by circulating salivary enzymes.
A 7-year-old client with infective endocarditis develops sudden-onset left ventricular failure, severe conduction blocks on ECG, and an unremitting fever despite 10 days of targeted antibiotic therapy. The nurse suspects the formation of which cardiac complication?
Explanation
Infective endocarditis progressioncan cause local extension of infection into adjacent perivalvular myocardial tissue.The structural breakdown of this fibrous skeleton triggersintracardiac abscess formation,particularly around the aortic root. This suppurative process destroys the conduction system and destabilizes the valvular anchoring architecture.
Rationale for correct answer:
2.A perivalvular ring abscessdirectly causes unremitting fever, severe conduction blocks, and sudden-onset heart failure.The anatomical proximity of the aortic valve ring to the atrioventricular node explains why abscess expansion precipitates atrioventricular conduction blocks.This localized pocket of infection remains shielded from systemic antimicrobials, explaining the persistent bacteremic feverdespite 10 days of targeted antibiotic therapy.
Rationale for incorrect answers:
1.A myocardial bridgeis a congenital structural variant where a segment of a coronary artery tunnels through the myocardium rather than resting on the epicardial surface. This anatomical anomaly can cause exertional ischemia or angina due to systolic arterial compression over a lifetime. However, it is entirely unrelated to infectious processes, acute valvular destruction, or unremitting febrile states.It does not present as an acute complication of active endovascular microbial colonization.
3.A coronary sinus aneurysmis an extremely rare vascular abnormality that is almost exclusively congenital in origin or secondary to chronic severe right atrial hypertension. It typically remains asymptomatic unless it causes localized compression or ruptures into an adjacent low-pressure cardiac chamber. It does not cause acute conduction disruptions, persistent fevers, or sudden left ventricular failureduring an active endocarditis episode. Its pathophysiology lacks any connection to suppurative valvular extension.
4.Pericardial effusion with tamponadecan occur during endocarditis but does not characteristically present with localized, severe progressive conduction blocks. Cardiac tamponade characteristically manifests with Beck triad, which includes hypotension, jugular venous distention, and muffled heart sounds, alongside low-voltage QRS complexes.While tamponade compromises filling pressures, it does not match the specific combination of localized atrioventricular nodal destructionand persistent focused fever seen here.
Test-taking strategy:
- Analyze the scenario/question: A 7-year-old child with infective endocarditis experiences sudden left ventricular failure, new conduction blocks on ECG, and an unremitting fever after 10 days of targeted antibiotics. The nurse must identify the underlying cardiac complication.
- Correlate symptoms with anatomy:
- Unremitting fever despite directed antibiotics indicates a walled-off, localized collection of pus that antibiotics cannot penetrate.
- New conduction blocks (such as prolonged PR interval or heart block) mean the infection has extended into the perivalvular tissue where the atrioventricular node and bundle of His reside.
- Evaluate choices:
- Rule inChoice 2:A perivalvular abscessexplains the structural valve failure, the conduction pathway disruption, and the antibiotic-resistant infectious fever pool.
- Rule outChoice 1:A myocardial bridge is a congenital anomalywhere an artery runs through muscle, which has no infectious or acute necrotic features.
- Rule outChoice 3:An aneurysm of the coronary sinus is a structural vascular defect that does not cause acute atrioventricular node destructionor high fevers.
- Rule outChoice 4:Pericardial tamponade restricts global cardiac filling and causes distant heart sounds,but it does not selectively destroy the central electrical conduction system.
Take home points
- A perivalvular ring abscess should be highly suspected in patients with endocarditis who develop new-onset conduction blocks or lengthening PR intervals.
- Persistent unremitting fever after a week of culture-directed antibiotic therapy indicates a localized, walled-off suppurative infection requiring surgical evaluation.
- Extension of endocarditis into the myocardial skeleton causes rapid structural valvular incompetence, leading to acute left-sided heart failure.
- Emergency surgical intervention is often required for perivalvular abscesses due to the extreme risk of myocardial rupture and complete heart block.
The nurse is preparing a family for home health nursing care as the child transitions to outpatient parenteral antimicrobial therapy (OPAT) for subacute endocarditis. Which discharge teachings are critical? Select all that apply
Explanation
Outpatient parenteral antimicrobial therapyrequires strict intravenous line managementto avoid central line-associated bloodstream infections. Safe home transitioning depends on impeccable aseptic technique maintenanceand parental vigilance for subtle decompensation signs. Managing prolonged therapy outside a hospital environment requires clear clinical escalation parameters.
Rationale for correct answers:
1.Daily inspection of the peripherally inserted central catheter line siteis critical for the early detection of localized infection or mechanical dislodgement.Families must be trained to recognize erythema, edema, induration, or purulent drainage, which indicate early exit-site infection. Prompt identification prevents local pathogens from migrating along the catheter tract into the central circulation, reducingcatheter-associated bacteremia risk.
2.Flushing the central line using sterile technique before and after medication administrationpreserves catheter patency and prevents luminal occlusionfrom blood clots or drug precipitates. Utilizing a strict aseptic approach prevents the inadvertent introduction of environmental pathogens into the central venous architecture. This practice minimizes the risk of secondary lines-related sepsis during prolonged parenteral therapy courses.
4.Reporting a return of fevers or poor feeding immediatelyis vital for catching potential treatment failure or a recurrent endovascular infection.New-onset pyrexia or lethargy in a pediatric patient can signal that the pathogen has developed resistance or that a new metastatic infectious focus has formed. Early clinical reporting allows providers to re-evaluate therapy parameters before hemodynamic decompensation occurs.
Rationale for incorrect answers:
3.Encouraging immediate participation in competitive contact sportsis strictly contraindicated for a child recovering from endocarditis with an active central line. Physical trauma can cause catheter fracturing, migration, or severe vascular laceration at the insertion site. Furthermore, the cardiac muscle requires rest to heal from inflammation, making strenuous physical exertion dangerous due to myocardial workload elevation.
5.Instructing families to double-dose oral antibiotics if an intravenous infusion is missedis an unsafe and incorrect clinical practice. Oral medications cannot achieve the high minimum inhibitory serum concentrations required to eradicate pathogens embedded within fibrin-platelet vegetations. Adjusting doses without provider oversight causes toxic serum fluctuations or inadequate pathogen suppression, directly compromisingantimicrobial stewardship principles.
Test-taking strategy:
- Analyze the scenario/question: A pediatric client with subacute endocarditis is transitioning to home health care for outpatient parenteral antimicrobial therapy (OPAT) via a PICC line. The nurse must identify all critical discharge teachings from a select-all-that-apply list.
- Determine Home Care Priorities:
- Protect the central venous access device from infection, occlusion, and displacement.
- Monitor the patient closely for clinical signs of infection recurrence or treatment failure.
- Maintain absolute safety restrictions regarding physical activity and medication compliance.
- Evaluate Choices:
- Rule inChoice 1:Monitoring the PICC sitedaily prevents minor insertion-site issues from progressing to severe systemic line infections.
- Rule inChoice 2:Flushing the line with sterile techniquemaintains catheter patency and blocks the entry of microbes into the bloodstream.
- Rule outChoice 3:Contact sports pose a massive risk for line dislodgementand put undue stress on a healing cardiovascular system.
- Rule inChoice 4:Reporting a return of feversensures immediate evaluation for potential treatment failure or line-associated sepsis.
- Rule outChoice 5:Families must never self-adjust regimens or swap intravenous infusionsfor oral double-dosing, which causes sub-therapeutic drug levels.
Take home points
- Daily visual inspection of the PICC line site is mandatory to detect early signs of localized exit-site infection or catheter migration.
- Central venous access lines must be flushed using strict aseptic technique before and after every medication delivery to maintain luminal patency.
- Pediatric patients undergoing outpatient intravenous therapy must avoid contact sports to prevent catheter damage and minimize cardiac workload.
- A return of fever, poor feeding, or increased lethargy are critical indicators of treatment failure that must be reported to the provider immediately.
The nurse is developing a nursing care plan for a pediatric client hospitalized with infective endocarditis during the acute phase of infection. Which interventions should the nurse prioritize? Select all that apply
Explanation
Acute phase managementfocuses on minimizing myocardial metabolic demandsand eradicating the causative bloodborne pathogens. Friable valvular vegetations pose a constant risk for systemic septic embolization.Comprehensive nursing vigilance targets the early detection of valvular structural incompetenceand subsequent hemodynamic decompensation.
Rationale for correct answers:
1.Enforcing strict bed rest reduces the metabolic workload of the heartand lowers overall cardiac output demands. Minimizing physical exertion protects fragile, inflamed endocardial structures from excessive hemodynamic shear stress. Restricting movement also decreases the risk of mechanical dislodgement of friable valvular vegetations, preventing catastrophic systemic embolic events.
3.Administering scheduled intravenous antibiotics exactly on timemaintains consistent, uninterrupted bactericidal serum concentrations. Maintaining high serum levels is essential for penetrating dense, avascular fibrin-platelet vegetative matrices.Delays in dosing can cause serum concentrations to fall below the minimum inhibitory concentration, allowing bacterial replication cyclesto resume.
4.Monitoring for tachycardia, tachypnea, and ralesallows for the early detection of acute congestive heart failure.Valvular destruction from tissue necrosis can trigger rapid hemodynamic failure and pulmonary venous congestion. Identifying these changes early enables prompt medical intervention with diuretics or afterload reducers before cardiogenic shock develops.
Rationale for incorrect answers:
2.Assisting with active range-of-motion exercisesis contraindicated during the acute, unstable phase of infective endocarditis. Increased physical activity elevates the heart rate and blood pressure, heightening myocardial shear stress. This mechanical stress significantly increases the risk of shearing off parts of fragile vegetations, leading to metastatic septic infarctions.
5.Restricting oral fluids to less than 500 mL per day regardless of weightis an unsafe and inappropriate intervention. Fluid management in pediatric patients must always be calculated precisely based on weight, body surface area, and systemic hydration status. Arbitrary, severe fluid restriction can cause profound intravascular dehydration, leading to hemoconcentration and increasing the risk of thromboembolic vascular occlusion.
Test-taking strategy:
- Analyze the scenario/question: The nurse is developing a nursing care plan for a pediatric client during the acute phase of infective endocarditis. The nurse must select the priority interventions from a select-all-that-apply list.
- Identify acute care priorities:
- Eradicate the infection through precise, consistent delivery of intravenous bactericidal agents.
- Reduce cardiac workload and prevent the mechanical dislodgement of friable valvular vegetations.
- Monitor closely for primary structural complications, specifically acute heart failure and pulmonary edema.
- Evaluate choices:
- Rule inChoice 1:Enforcing strict bed restis essential during the acute phase to lower cardiac output and minimize embolic risks.
- Rule outChoice 2:Range-of-motion exercises increase physical exertion and elevate the hazard of vegetation fragmentation.
- Rule inChoice 3:Delivering intravenous antibioticsprecisely on schedule prevents sub-therapeutic serum troughs that compromise bacterial clearance.
- Rule inChoice 4:Tracking tachycardia and ralesprovides an early warning sign of acute valvular failure and fluid backup.
- Rule outChoice 5:Implementing an uncalculated fluid restrictionviolates pediatric safety rules and risks severe intravascular volume depletion.
Take home points
- Strict bed rest is mandatory during the acute phase of endocarditis to reduce cardiac workload and minimize the risk of vegetation embolization.
- Intravenous antibiotics must be administered precisely on schedule to maintain serum levels above the minimum inhibitory concentration.
- Frequent monitoring for tachycardia, tachypnea, and pulmonary rales is critical to detect the onset of acute congestive heart failure.
- Pediatric fluid restrictions must always be customized based on weight and clinical status rather than applying fixed, arbitrary limits.
Comprehensive Questions
A client is admitted with a diagnosis of acute infective endocarditis (IE). Which findings during a nursing assessment support this diagnosis? Select all that apply
Explanation
Acute infective endocarditisis a severe microbial infection of the endocardium,typically involving the valves. It causes valvular destruction, vegetative embolization, and immune complex deposition. Highfeverand virulent bacteremia are characteristic.
Rationale for correct answers:
1.Skin petechiaeare common vascular manifestations of infective endocarditis. They result from microembolization of vegetative fragmentsor localized immune-mediated vasculitis.This finding provides crucial physical evidence of systemic capillary damage.
2.Crackles at the lung basesindicate pulmonary congestion from left-sided heart failure.Valvular incompetence due to rapid tissue destruction impairs forward blood flow. This leads to acute pulmonary fluid volume overload.
3.Peripheral edemaindicates fluid retention secondary to right-sided heart failure.Valvular dysfunction disrupts normal hemodynamics, leading to systemic venous congestion. This symptom reflects advancing hemodynamic instability in acute cases.
4.A newly developed or changing cardiac murmuris a hallmark clinical sign. It signifies turbulent blood flowacross damaged, eroding endocardial valves.This finding directly reflects acute structural valvular destruction.
5.Arthralgiaoccurs frequently due to circulating immune complex deposition in the joints.This immunological phenomenon causes localized inflammation and significant joint pain. It represents a common systemic manifestation of this infectious process.
Rationale for incorrect answers:
6.A decreased erythrocyte sedimentation rateis incorrect because infective endocarditis triggers a profound systemic inflammatory response. The erythrocyte sedimentation rate will be significantly elevated, not decreased, along with C-reactive protein. This lab value reflects active, ongoing intravascular infection.
Test-taking strategy:
- Analyze the scenario/question: The patient has acute infective endocarditis, a destructive bacterial infection of the inner heart lining. The nurse must identify physical signs, complications, and lab findings that support this specific diagnosis.
- Evaluate clinical manifestations:
- Choice 1is correct because microemboli cause petechiae.
- Choice 4is correct because vegetative lesions distort valves, creating new murmurs.
- Choice 5is correct because immune complexes cause arthralgia.
- Identify complications:
- Choice 2and Choice 3are correct because acute valvular damage rapidly precipitates heart failure, leading to pulmonary congestion and peripheral fluid retention.
- Apply pathophysiology:
- Rule out Choice 6because systemic infections cause an elevated, not decreased, erythrocyte sedimentation rate due to increased acute-phase reactants.
Take home points:
- Infective endocarditis presents with vascular and immunologic signs like petechiae, Janeway lesions, Osler nodes, and arthralgia.
- Structural valve destruction often leads to a new murmur and rapid-onset heart failure manifested by crackles and edema.
- Inflammatory markers such as erythrocyte sedimentation rate and C-reactive protein are characteristically elevated in this disease.
- Acute infective endocarditis is differentiated from the subacute form by its sudden onset, high fever, and rapid cardiac tissue destruction.
The nurse is conducting a staff education program on infective endocarditis. Which of the following statements about infective endocarditis are correct?
Explanation
Infective endocarditisis a microbial infection of theendocardiumthat primarily targets cardiac valves. It arises from endothelial damage, plate-fibrin deposition, and bacteremia, leading to vegetations. High-velocity blood flowthrough congenital or acquired defects accelerates this destructive process.
Rationale for correct answers:
2.Staphylococcus aureusis the leading causative organism in acute infective endocarditis. It is highly virulent and capable of infecting normal heart valves. This pathogen causes rapid, severe valvular destructionand systemic embolic complications.
3.Antibiotic prophylaxisis indicated before high-risk procedures involving the respiratory mucosa for susceptible individuals. Preventing bacteremia during surgical manipulation of the ear, nose, and throat reduces endothelial seeding. This is a vital preventative strategy in high-risk patients.
4.Body tattooingintroduces a direct portal of entry for skin flora into the bloodstream. This transient bacteremiacan cause subacute bacterial endocarditis on vulnerable or damaged endocardial surfaces. It represents a significant behavioral risk factor for contamination.
5.A prolonged, unexplained feveris the most common clinical manifestation of this infection. The continuous release of pyrogens from intravascular vegetative lesions sustains the febrile state. This finding serves as a key diagnostic indicator during evaluation.
Rationale for incorrect answers:
1.Infective endocarditis is unlikely to occur with ventricular septal defect is incorrect because high-velocity jet streams create severe endothelial turbulence. Ventricular septal defects actually carry a high risk for bacterial colonizationand vegetation formation. This structural abnormality significantly increasesendocardial susceptibilityto infection.
Test-taking strategy:
- Analyze the scenario/question: The nurse is identifying correct epidemiological, pathophysiological, and preventative facts regarding infective endocarditis to educate nursing staff.
- Evaluate risk factors and etiology:
- Choice 2is correct because staphylococcal species are the primary cause of acute intravascular infections.
- Choice 4is correct because breaking the skin barrier via tattooing introduces virulent pathogens directly into circulation, risking subacute bacterial endocarditis.
- Apply prophylaxis guidelines:
- Choice 3is correct because surgical manipulation of the respiratory tract requires antibiotic coverage in patients with high-risk cardiac conditions.
- Assess clinical presentation:
- Choice 5is correct because a persistent, prolonged fever is the hallmark sign of continuous bacteremia.
- Examine pathophysiology:
- Rule out Choice 1because high-velocity congenital shunts like ventricular septal defects create turbulent flows that heavily predispose the endocardium to bacterial seeding.
Take home points:
- High-velocity congenital heart defects like ventricular septal defects increase the risk of endothelial damage and subsequent bacterial colonization.
- Staphylococcus aureus is the most common and destructive pathogen responsible for acute infective endocarditis cases worldwide.
- Antimicrobial prophylaxis is recommended prior to invasive respiratory procedures for individuals with pre-existing high-risk cardiac lesions.
- Intravenous drug use, body piercings, and tattoos are prominent entry portals for skin bacteria to cause endocardial infections.
A child with congenital heart disease needs prophylactic antibiotics to prevent infective endocarditis in the following circumstances:
Explanation
Infective endocarditis prophylaxistargets specific high-riskcardiac substratesexposed to bacteremia-inducing procedures. Transient bacteremia occurs heavily during manipulation of gingival tissue or periapical regions. Guidelines restrict antimicrobial administrationto select interventions to avoidresistance.
Rationale for correct answer:
1.Dental proceduresinvolving manipulation of gingival tissue, the periapical region of teeth, or perforation of the oral mucosa require prophylaxis. These interventions introduce high loads of viridans group streptococciinto the bloodstream. This selective pre-treatmentforms the foundation of infective endocarditis prevention.
Rationale for incorrect answers:
2.A skin lacerationis an accidental, minor traumathat does not warrant routine systemic antibiotic prophylaxis for endocarditis prevention. Standard wound care and localized cleansing are sufficient to prevent localized pyogenic complications. Routine systemic coverage for simple cutaneous breaks is strictly avoided to prevent drug toxicity.
3.Tonsillitisis an acute inflammatory and infectious condition that requires appropriate therapeutic antibiotics rather than short-term procedural prophylaxis. Endocarditis prevention protocols are specifically designed for transient bacteremia caused by mechanical instrumentation, not localized viral or bacterial parenchymal infections. Treating the active infection directly eliminates the bacterialload over time.
4.Measlesis an acute viral exanthem caused by a morbillivirus that does not induce bacterial seeding of the endocardium. Antibiotics are completely ineffective against viral pathogens and play no role in preventing endocarditis during viral illnesses. Management focuses purely on supportive care and immunization strategies.
Test-taking strategy:
- Analyze the scenario/question: The nurse must determine which clinical scenario requires the administration of prophylactic antibiotics to prevent infective endocarditis in a pediatric patient with congenital heart disease.
- Apply evidence-based guidelines:
- Choice 1is correct because modern clinical guidelines restrict infective endocarditis prophylaxis almost exclusively to high-risk dental procedures that disrupt the oral mucosa.
- Distinguish trauma from instrumentation:
- Rule out Choice 2because clean or minor skin lacerations do not meet the threshold for systemic pre-procedural prophylaxis.
- Identify pathology:
- Rule out Choice 3and Choice 4because treating an established respiratory infection or managing a viral exanthem requires therapeutic or supportive regimens, not procedural prophylaxis.
Take home points:
- Antibiotic prophylaxis for infective endocarditis is strictly indicated for dental procedures that involve the manipulation of gingival tissue or periapical segments.
- Routine prophylaxis is not recommended for simple, non-surgical cutaneous wounds or accidental minor lacerations.
- Only specific high-risk cardiac conditions, such as prosthetic valves or unrepaired cyanotic congenital heart defects, require procedural prophylaxis.
- Good oral hygiene and regular dental care are more effective at reducing the risk of endocarditis than procedural antibiotic cover.
A client has an admitting diagnosis of acute left-sided infective endocarditis. What is the best test to confirm this diagnosis?
Explanation
Infective endocarditis confirmationnecessitates isolating pathogens via bactericidalculture profiles.Persistent bacteremia from Streptococcus mutansdamages tissue, manifesting as pyrexia, glomerulonephritis, and pathognomonicvascular emboli.
Rationale for correct answer:
1.Blood culturesprovide definitive microbiological confirmationof continuous bacteremia. Isolating the causative microorganism allows for targeted antibiotic susceptibility profiling. Sustained positive results satisfy a major requirement of the Duke criteria. This remains the absolute diagnostic standard for endovascular infections.
Rationale for incorrect answers:
2.A complete blood countprovides supportive evidenceof inflammation but cannot confirm endocarditis. Leukocytosis and normocytic anemia are highly non-specific findingscommon to many systemic infections. This laboratory panel lacks the capacity to isolate specific endovascular pathogens. It can only track general hematologic responses during active disease phases.
3.Cardiac catheterizationis an invasive hemodynamic procedurenot used for routine endocarditis confirmation. It carries an extremely high risk of mechanically dislodging fragilevalvular vegetations. This risk can precipitate catastrophic systemic embolic strokes or peripheral infarctions. It is reserved strictly for evaluating coronary anatomy before urgent surgical intervention.
4.A transesophageal echocardiogramis a highly sensitive imaging modality but does not confirm microbiological identity.It visualizes structural damage, valvular regurgitation, and oscillating endocardial masses perfectly. While satisfying a major imaging criterion, it cannot differentiate infectious vegetations from sterile thrombi. It must always be paired with microbial cultures for definitive diagnostic confirmation.
Test-taking strategy:
- Analyze the scenario/question: The question asks for the most definitive diagnostic test required to confirm a suspected diagnosis of infective endocarditis.
- Apply diagnostic standards:
- Definitive confirmation of endovascular infection requires isolating the specific microorganism from the bloodstream.
- Imaging and general laboratory tests provide structural or inflammatory evidence but lack microbiological specificity.
- Evaluate choices:
- Rule inChoice 1:Drawing blood culturesprovides the definitive microbiological confirmation required by the clinical diagnostic criteria.
- Rule outChoice 2:A complete blood countshows general inflammatory markers like leukocytosis but cannot isolate the causative pathogen.
- Rule outChoice 3:Conducting cardiac catheterizationis contraindicated for routine diagnosis due to the high risk of shearing off vegetations.
- Rule outChoice 4:A transesophageal echocardiogramprovides excellent anatomical visualization but cannot establish a definitive microbiological profile.
Take home points
- Positive blood cultures serve as the primary major criterion for confirming a diagnosis of infective endocarditis.
- A complete blood count typically demonstrates leukocytosis and normocytic anemia but lacks the specificity required for diagnosis.
- Echocardiography is utilized to visualize anatomical vegetations and valvular function but cannot establish microbiological identity alone.
- Invasive cardiac catheterization is avoided during the acute phase due to the severe risk of causing septic embolization.
The nurse is conducting a staff education program on infective endocarditis. Which manifestation of infective endocarditis is a result of fragmentation and microembolization of vegetative lesions?
Explanation
Vascular phenomenain infective endocarditis manifest due to distinct pathophysiological mechanisms. Microembolizationinvolving fragmented vegetative lesions physically occludes terminal capillaries. Conversely, other cutaneous and ocular signs stem from localized, immune complex-mediated hypersensitivity vasculitisrather than mechanical thromboembolism.
Rationale for correct answer:
1.Petechiaeare small, macular hemorrhages resulting directly from microembolization of vegetative fragments to the capillaries.These fragments physically disrupt the endothelial lining, causing localized extravasation of RBCs into the dermis. This makes them a direct vascular manifestation of mechanical emboli.
Rationale for incorrect answers:
2.Roth’s spotsare oval, pale-centered retinal hemorrhagesthat are caused by an immunological phenomenonrather than mechanical microembolization. They occur when circulating antigen-antibody complexes deposit within the ocular microvasculature, triggering a localized perivascular hypersensitivity reaction. This distinguishes them as a purely immunologic signof the disease.
3.Osler’s nodesare painful, tender, erythematous nodules typically found on the pads of the fingers and toes.They are caused by immune complex deposition in the dermal vessels, which incites an inflammatory perivascular response. They are classified as immunologic lesions rather than results of vegetative lesion fragmentation.
4.Splinter hemorrhagesare linear, dark-red streaks appearing under the nail beds,caused primarily by immunologic microvascular inflammation.While historically debated, modern pathophysiology attributes these lesions predominantly to immune-mediated capillary vasculitis rather than direct fragmentation of cardiac vegetations. Thus, they represent localized immune-mediated damagerather than migratory emboli.
Test-taking strategy:
- Analyze the scenario/question: The nurse is educating staff on the manifestations of infective endocarditis, specifically looking for the sign caused directly by fragmentation and microembolization of vegetative lesions.
- Differentiate pathophysiology:
- Choice 1is correct because petechiae are classic vascular phenomena directly resulting from the mechanical breaking off and migration of small vegetative particles.
- Distinguish vascular from immunologic:
- Rule out Choice 2and Choice 3because Roth's spots and Osler's nodes are explicitly classified as immunologic manifestations under the Duke criteria, driven by type three hypersensitivity reactions.
- Evaluate microvascular lesions:
- Rule out Choice 4because splinter hemorrhages are predominantly caused by capillary vasculitis under the nails rather than migrating macro- or micro-thrombi from endocardial valves.
Take home points:
- Clinical signs of endocarditis are strictly divided into vascular phenomena and immunologic phenomena under the diagnostic Duke criteria.
- Petechiae, systemic arterial emboli, splenic long-range infarctions, and Janeway lesions represent the mechanical vascular consequences of fragmenting vegetations.
- Osler's nodes, Roth's spots, glomerulonephritis, and rheumatoid factor elevation are consequences of circulating antigen-antibody complex tissue deposition.
- Vascular embolic phenomena from left-sided infective endocarditis present a high risk for ischemic stroke, myocardial infarction, and mesenteric ischemia.
The nurse is caring for a 16-year-old client with infective endocarditis. What describes Janeway’s lesions that are manifestations of this disease?
Explanation
Vascular and immunologic phenomenamust be accurately differentiated during clinical assessments for infective endocarditis. Certain cutaneous lesions manifest as flat, insensitive markings resulting from septic microemboli that induce focal necrosis.These distinct macules typically appear on peripheral glabrous skin surfaces, serving as a critical diagnostic marker for endocardial seeding.
Rationale for correct answer:
4.Janeway's lesionsare flat, erythematous, painless macules located on the palms of the hands and soles of the feet.They represent acute vascular phenomena caused by septic microembolizationfrom valvular vegetations, leading to localized dermal microabscesses and necrosis. Their lack of tenderness is a defining pathognomonic feature that supports the diagnosis.
Rationale for incorrect answers:
1.Hemorrhagic retinal lesionsdescribe Roth's spots, which are immunologic phenomenarather than vascular skin lesions. They present as round or oval retinal hemorrhages with pale, white centers consisting of fibrin-platelet thrombi surrounded by exudate. This distinct finding requires an ophthalmoscopic examination to visualize intracular inflammation.
2.Black longitudinal streaks in nail bedsdefine splinter hemorrhages,which occur in the subungual capillary beds. They run vertically along the longitudinal axis of the nail and are primarily caused by microvascular inflammation or localized vasculitis. While useful signs, they do not match the physical or anatomical description of Janeway's macules.
3.Painful red or purple lesions on fingers or toesdescribe Osler's nodes,which are immunologicrather than embolic phenomena. These raised, tender nodules develop on the pads of the digits due to localized immune complex deposition and subsequent perivascular hypersensitivity. Their prominent pain and swelling contrast directly with painless vascularfindings.
Test-taking strategy:
- Analyze the scenario/question: The nurse is assessing a adolescent client with infective endocarditis. The question asks for the specific physical description and location that defines Janeway's lesions.
- Differentiate cutaneous manifestations:
- Choice 4is correct because Janeway's lesions are specifically flat, red, and completely painless spots located exclusively on the palms and soles.
- Distinguish physical features:
- Rule out Choice 3because painful, raised digital nodules describe Osler's nodes, which are immunologic, whereas Janeway's are vascular and painless.
- Identify anatomical sites:
- Rule out Choice 1because retinal hemorrhages describe Roth's spots.
- Rule out Choice 2because linear subungual streaks describe splinter hemorrhages.
Take home points:
- Janeway's lesions are flat, red, painless macules on the palms and soles caused by septic microembolization and focal dermal necrosis.
- Osler's nodes are raised, purple, highly painful nodules on the pads of fingers and toes caused by immune complex hypersensitivity.
- Splinter hemorrhages present as vertical, dark-red or black lines beneath the nail plates due to microvascular capillary damage.
- Under the modified Duke criteria, Janeway's lesions are classified as vascular phenomena, whereas Osler's nodes are classified as immunologic phenomena.
A client with infective endocarditis of a prosthetic mitral valve develops a left hemiparesis and visual changes. What should the nurse expect to be included in collaborative management of the client?
Explanation
Septic embolizationconstitutes a critical manifestation of prosthetic valve endocarditis, frequently targeting the cerebral vascular tree.Large, friable vegetations on mechanical hardware resist sterilization and demonstrate a high propensity for mechanical fragmentation. When antimicrobial therapy fails to suppress embolic risks, urgent surgical debridementbecomes necessary to protect neurological structures and restore valvular integrity.
Rationale for correct answer:
2.Surgical valve replacementis indicated for prosthetic valve endocarditis complicated by recurrent systemic embolizationand progressive neurological deficits. The development of left hemiparesis and visual changes signals a septic embolic strokeoriginating from the mitral hardware. Operative intervention removes the infectious vegetation nidus, preventing further ischemic tissue damage. Replacing the compromised prosthesis is the definitive method to achieve hemodynamic stabilization when medical therapy alone cannot control embolic shedding.
Rationale for incorrect answers:
1.A mechanical embolectomyis an emergency intervention used to clear acute large-vessel occlusions, but it does not address the underlying source of infection. Performing a peripheral or cerebral thrombectomy without resolving the valvular source leaves the client exposed to immediate recurrent embolic fragmentation.Surgical attention must prioritize removing the primary intracardiac vegetation pool over isolated peripheral vascular clearing.Therefore, embolectomy is considered a secondary, adjunctive measure rather than the primary collaborative solution.
3.Administering therapeutic anticoagulantsis contraindicated in acute infective endocarditis due to the high risk of catastrophic intracerebral hemorrhage.Septic emboli damage the structural integrity of the cerebral arterial wall, predisposing the vessel to mycotic aneurysm formation.Introducing anticoagulation can turn a bland ischemic infarct into a fatal intracranial hemorrhagic transformation. Standard guidelines mandate holding or avoiding anticoagulants during the acute, unstable phase of endovascular infections.
4.Prescribing higher than usual antibiotic dosagesis an incorrect strategy because endocarditis regimens are already optimized at maximal bactericidal thresholds. Antimicrobial delivery is carefully calibrated to achieve peak serum levels that penetrate dense, avascular fibrin-platelet matrices. Exceeding these standardized, high-dose ceilings does not accelerate vegetative clearance or prevent mechanical shearing of clots. Instead, escalating doses beyond established guidelines primarily increases the risk oforgan-system toxicitywithout altering embolic risk profiles.
Test-taking strategy:
- Analyze the scenario/question: A client with prosthetic mitral valve infective endocarditis exhibits a left hemiparesis and visual changes. The nurse must identify the primary collaborative management intervention based on a provided correct answer of choice 2.
- Evaluate clinical complications:
- Left hemiparesis and visual changes indicate an acute embolic stroke involving the right cerebral hemisphere and visual pathways.
- Prosthetic valve endocarditis with systemic embolic complications represents a clear indication for urgent surgical intervention.
- Evaluate choices:
- Rule inChoice 2:A valve replacementis the definitive treatment to remove the vegetative source, preventing further stroke progression and restoring cardiac function.
- Rule outChoice 1:An isolated embolectomyhandles the immediate vascular block but leaves the primary cardiac source active and capable of re-embolizing.
- Rule outChoice 3:Implementing anticoagulation therapyis dangerous because it risks converting an ischemic embolic stroke into a major hemorrhagic event.
- Rule outChoice 4:Elevating antibiotic dosagesbeyond standard max limits provides no mechanical stability to friable clots and risks severe systemic toxicity.
Take home points
- Surgical valve replacement is the definitive collaborative intervention for prosthetic valve endocarditis complicated by systemic embolic strokes.
- New-onset neurological deficits like hemiparesis indicate that friable valvular vegetations have fragmented and traveled to the cerebral circulation.
- Therapeutic anticoagulation is strictly avoided in acute infective endocarditis due to the risk of inducing an intracranial hemorrhage.
- Antimicrobial therapy for endocarditis is always initiated at maximal bactericidal doses, meaning dose escalation cannot substitute for surgical removal.
A client with aortic valve endocarditis develops dyspnea, crackles in the lungs, and restlessness. What should the nurse suspect that the client is experiencing?
Explanation
Aortic valve endocarditiscarries an extreme risk for rapid, destructive structural damage. Bacterial vegetations erode and perforate the valve leaflets, causing acute aortic regurgitation. This massive backward flow overloads the left ventricle, causing back-up pressure into the lungs. The resulting pulmonary congestionleads to severe hypoxemia and rapid hemodynamic collapse.
Rationale for correct answer:
3.Valvular incompetence with resulting heart failureis the primary cause of acute dyspnea and cracklesin aortic endocarditis. Leaflet destruction prevents proper valve closure during diastole, causing massive blood volume to reflux back into the left ventricle. This rapidly elevates left atrial and pulmonary venous pressures, driving alveolar transudationand respiratory distress.
Rationale for incorrect answers:
1.Pulmonary embolizationfrom valve vegetations is incorrect because left-sided cardiac lesions embolize into the systemic arterial circulation, not the lungs. For a vegetation to reach the pulmonary vasculature, it must originate from a right-sided structure like the tricuspid valve. Therefore, an aortic lesion cannot physically cause a pulmonary embolism.
2.Vegetative embolization to the coronary arteriesis an uncommon complication that typically presents as an acute myocardial infarction. The patient would exhibit crushing, substernal chest pain, ischemic electrocardiogram changes, and elevated cardiac biomarkers. While it causes cardiogenic shock, it does not explain isolated, progressive bilateral pulmonary fluid congestion.
4.Nonspecific manifestations that accompany infectious diseasesis incorrect because acute dyspnea, basilar crackles, and restlessness signify organ dysfunction. These are hard physical signs of respiratory failure and cardiac decompensation, not generalized constitutional symptoms like malaise. Labeling these findings as non-specific risks delaying lifesaving emergency interventions.
Test-taking strategy:
- Analyze the scenario/question: The patient has aortic valve endocarditis (a left-sided heart infection) and develops acute dyspnea, crackles, and restlessness. The nurse must identify the underlying pathophysiology.
- Trace hemodynamics and anatomy:
- Choice 3is correct because the aortic valve is on the left side of the heart. Destruction of this valve causes acute regurgitation, left ventricular volume overload, and backward failure into the lungs, producing crackles.
- Apply circulatory pathways:
- Rule out Choice 1because left-sided emboli travel to the brain and systemic organs, whereas right-sided emboli travel to the lungs.
- Differentiate presentations:
- Rule out Choice 2because coronary embolization causes acute myocardial infarction presenting primarily with chest pain and ST-segment elevations rather than isolated pulmonary edema.
- Rule out Choice 4because crackles and dyspnea are specific signs of fluid in the alveoli, never general infection symptoms.
Take home points:
- Acute heart failure secondary to valvular incompetence is the most frequent and life-threatening complication of aortic infective endocarditis.
- Left-sided endocarditis vegetations embolize systemically to organs like the brain, spleen, and kidneys, never into the pulmonary artery.
- Restlessness and anxiety are early, sensitive behavioral indicators of cerebral hypoxia caused by declining cardiac output and pulmonary congestion.
- Rapidly developing aortic regurgitation causes a dramatic rise in left ventricular end-diastolic pressure, leading to flash pulmonary edema.
A client hospitalized for 1 week with subacute infective endocarditis is afebrile and has no signs of heart damage. Discharge with outpatient antibiotic therapy is planned. During discharge planning with the client, what is it most important for the nurse to do?
Explanation
Discharge planning for a client with subacute infective endocarditisrequiring long-term outpatient intravenous antibiotic therapy centers on safety and continuity of care.Eradication of endocardial vegetations demands continuous adherence to strict therapeutic regimens over 4 to 6 weeks.The nurse must verify that the domestic setting possesses the infrastructure to support a central venous access device, safely manage intravenous infusions, and handle medical emergencies.
Rationale for correct answer:
4.Assessing the home environment, family support networks, and geographic accessto medical facilities is the highest priority before discharge. Outpatient intravenous antibiotic therapy requires a stable domestic infrastructure, reliable refrigeration for medications, clean running water, and an intelligent caregiver to mitigate the risks of line sepsis or catheter dislodgement.Furthermore, proximity to a hospital ensures rapid interventionif the client develops acute valvular failure.
Rationale for incorrect answers:
1.Planning how needs will be metwhile continuing on bed restis incorrect because absolute bed rest is not indicated for a stable, afebrile client with no structural heart damage. Prolonged, unnecessary immobilization heavily increases the risk of deep vein thrombosis, muscular atrophy, and atelectasis. Clients are encouraged to engage in progressive, moderate ambulationas toleratedto maintain functional status.
2.Encouraging the use of diversional activities to relieve boredom and restlessnessis a supportive nursing action but does not address critical safety and physiological needs. While psychological well-being is important during long-term therapy, it is secondary to establishing vascular access safety and confirming emergency protocols. Psychological comfort measures are prioritized only after environmental safetyis fully secured.
3.Teaching the client to avoid crowds and exposure to upper respiratory infectionsis a general health recommendation that lacks specificity for endocarditis pathophysiology. Subacute infective endocarditis is primarily driven by slow-growing skin or oral microflora, such as viridans group streptococci, rather than airborne respiratory pathogens. While preventing illness is beneficial, this intervention does not protect against vascular access contaminationor recurrence.
Test-taking strategy:
- Analyze the scenario/question: A client who has been stable for 1 week with subacute endocarditis is being discharged to finish long-term outpatient intravenous antibiotic therapy at home. The nurse must identify the most important discharge action.
- Prioritize based on safety:
- Choice 4is correct because outpatient intravenous therapy carries severe risks of line sepsis and requires complex daily management; the home environment and support system must be evaluated first to ensure the therapy can be safely completed.
- Eliminate misconceptions:
- Rule out Choice 1because strict bed rest is contraindicated and unnecessary for an afebrile patient without heart failure.
- Differentiate hierarchy of needs:
- Rule out Choice 2because diversional activities address a non-urgent psychosocial need, whereas environmental readiness addresses physiological safety.
- Evaluate pathophysiological relevance:
- Rule out Choice 3because avoiding respiratory infections is less relevant to endocarditis management than ensuring compliance and monitoring for embolic or infectious line complications.
Take home points:
- Successful outpatient management of infective endocarditis requires several weeks of regular central venous catheter care and strict antibiotic adherence.
- Comprehensive assessment of family support and proximity to emergency care is mandatory to manage potential complications like line sepsis or embolization.
- Complete bed rest is avoided in stable endocarditis patients to prevent deconditioning and thromboembolic events, allowing for mild to moderate activity.
- Home health nurses collaborate with families to monitor for red-flag symptoms, including recurrent fevers, dyspnea, and sudden neurological changes.
The nurse is providing discharge education to a 17-year-old client with infective endocarditis. Which of the following instructions should the nurse provide on how to prevent recurrence of the infection?
Explanation
Preventing the recurrence of infective endocarditisis a lifelong priority for individuals who have survived an initial episode, as their damaged endocardial surfaces are highly susceptible to bacterial adhesion. Transient bacteremiacan occur during everyday activities but is significantly elevated during specific mechanical disruptions of the mucosa. Targeted pharmacological prophylaxisremains the established standard for mitigating this risk during high-risk exposures.
Rationale for correct answer:
4.Obtaining prophylactic antibiotic therapybefore certain invasive medical or dental proceduresis the correct method to prevent recurrence. A prior history of infective endocarditis places the client in the highest-risk category according to American Heart Association guidelines, requiring pre-procedural amoxicillin or clindamycin.This targeted pre-treatment effectively neutralizes transient bacteremiabefore organisms can colonize vulnerable cardiac endothelium.
Rationale for incorrect answers:
1.Starting on antibiotic therapy when exposed to persons with infectionsis incorrect because endocarditis is caused by autologous skin or oral flora entering the bloodstream, not by casual exposure to contagious illnesses. Administering antibiotics for general viral or respiratory exposures is inappropriate and contributes heavily to drug resistance. Prevention focuses on procedural barriers rather than avoiding community illnesses.
2.Taking one aspirin a day to prevent vegetative lesions from forming around the valvesis incorrect because antiplatelet therapy does not prevent or treat bacterial colonization of the endocardium. Clinical trials have demonstrated that aspirin does not reduce vegetation size or embolic risk in endocarditis, and it significantly increases the hazard of internal hemorrhage. Management relies strictly on bactericidal antimicrobials, not antiplatelet agents.
3.Always maintaining continuous antibiotic therapyto prevent the development of any systemic infection is incorrect and dangerous. Continuous, indefinite systemic antibiotic administration induces severe bone marrow suppression, organ toxicity, and the selection of multi-drug resistant superbugs. Antibiotics are strictly reserved for targeted, short-term pre-procedural prophylaxis rather than permanent suppressive regimens.
Test-taking strategy:
- Analyze the scenario/question: A 17-year-old client is being discharged after recovering from infective endocarditis. The nurse must identify the correct evidence-based instruction to prevent a recurrence of the disease.
- Apply professional guidelines:
- Choice 4is correct because a previous history of infective endocarditis is an absolute indication for prophylactic antibiotics prior to dental cleanings or procedures manipulating the gingival margins.
- Identify pharmacological misconceptions:
- Rule out Choice 2because aspirin and anticoagulants have no preventive efficacy against bacterial vegetations and increase the risk of bleeding.
- Rule out excessive or inappropriate therapy:
- Rule out Choice 1because endocarditis is not caught from people with standard communicable infections.
- Rule out Choice 3because continuous, lifelong antibiotic therapy is contraindicated due to toxicities and resistance risks.
Take home points:
- A previous history of infective endocarditis is a primary high-risk indication requiring lifetime pre-procedural antibiotic prophylaxis for specific dental interventions.
- Maintaining meticulous, daily oral hygiene and scheduling regular dental evaluations reduces the incidence of spontaneous low-grade bacteremia more than prophylactic drugs.
- Antiplatelet agents like aspirin play no role in preventing endocardial vegetation growth and are avoided due to increased risks of bleeding.
- High-risk individuals should completely avoid body piercings, tattooing, and any unnecessary non-sterile skin penetrations to minimize bacterial access to the circulation.
The nurse is assessing a 17-year-old client with infective endocarditis suspected of IV cocaine use. Which of the following signs and symptoms should the nurse anticipate? Select all that apply
Explanation
Intravenous drug abuseinduces endocarditis via direct endothelial inoculation of Staphylococcus aureus, frequently targeting the tricuspidvalve. This intravascular infection causes destructive vegetations, septic thromboemboli, structural valvular incompetence, and widespread immune complex vasculitis, presenting with persistent bacteremia.
Rationale for correct answers:
1.Retinal hemorrhages,known as Roth's spots,represent immunologic phenomena in endocarditis. They occur when circulating antigen-antibody complexes deposit in the ocular microvasculature, causing localized perivascular inflammation. This produces a characteristic pale-centeredhemorrhagic lesionseen on fundoscopic examination.
2.Splinter hemorrhagesmanifest as dark, linear streaks beneath the nail beds.They result from microvascular inflammation or microembolization within the subungual capillaries. This classical finding provides visible physical evidence of underlying vascular damage during systemic endocardial infection.
3.Osler's nodesare painful, erythematous, raised nodules typically found on the pads of digits.They represent a classic immunologic phenomenon triggered by localized immune complex deposition. This inciting event causes a tender hypersensitivity reaction within the peripheral dermal vessels.
5.Janeway's lesionsare flat, red, painless macules appearing on the palms and soles.They are vascular phenomena caused by septic microembolization from cardiac vegetations. These migrating emboli induce focal endothelial necrosis and small microabscess formations within glabrous cutaneous tissues.
Rationale for incorrect answers:
4.Painless nodules over bony prominencesdescribe subcutaneous nodules,which are characteristic of rheumatic fever rather than endocarditis. These collagenous aggregations occur via a separate autoimmune mechanism following group A streptococcal pharyngitis. They reflect rheumatic carditis instead of active intravascular seeding.
Test-taking strategy:
- Analyze the scenario/question: The client is an adolescent with infective endocarditis secondary to suspected intravenous drug use, which frequently introduces skin pathogens into the venous system. The nurse must identify vascular and immunologic assessment findings associated with this diagnosis.
- Differentiate clinical syndromes:
- Choice 1, Choice 2, Choice 3,and Choice 5are correct because they represent classic clinical signs of infective endocarditis included in the modified Duke criteria.
- Identify Choice 1, Choice 3,and Choice 2as manifestations driven by immune complex deposition or capillary microembolization that can occur globally.
- Recognize Choice 5as a pathognomonic embolic event unique to endocardial vegetation shedding.
- Examine exclusions:
- Rule out Choice 4because painless nodules over bony joints point directly to Jones criteria for acute rheumatic fever.This structural lesion does not occur from direct microbial colonizationof the valves.
Take home points:
- Infective endocarditis secondary to intravenous drug use predominantly affects the tricuspid valve but can still cause systemic vascular and immunologic phenomena.
- Vascular signs include splinter hemorrhages, petechiae, and painless Janeway's lesions, which result from mechanical microembolization of vegetative fragments.
- Immunologic signs include painful Osler's nodes and retinal Roth's spots, which are driven by circulating antigen-antibody complex tissue deposition.
- Subcutaneous nodules over bony prominences are specific to acute rheumatic fever and do not serve as diagnostic indicators for endocarditis.
The nurse is preparing to draw blood cultures for a pediatric client with suspected infective endocarditis. Which action must the nurse implement to ensure diagnostic accuracy?
Explanation
Accurate microbiological identificationforms the cornerstone of managing infective endocarditis, as treatment relies on matching specific targeted bactericidal agents to the causative pathogen. Because endocarditis produces continuous, low-grade bacteremia rather than transient spikes, isolation of the organism depends on volume and sampling distribution. Implementing precise collection protocols preventssample contaminationand avoids false-negative results,ensuring patientdiagnostic safety.
Rationale for correct answer:
2.Obtaining at least three separate blood culturesfrom different peripheral venipuncture sites is the mandatory standard to confirm continuous bacteremia. Sampling from multiple independent anatomical locations allows clinicians to differentiate true intravascular pathogens from common skin contaminantslike coagulase-negative staphylococci. If all separate cultures grow the same organism, it provides the major Duke criterion necessary for an indisputable endocarditis confirmation.
Rationale for incorrect answers:
1.Drawing all blood samples from a single indwelling central line within 10 minutesis incorrect and compromises sample integrity. Indwelling catheters are frequently colonized by biofilms, which leads to falsely positive results that do not reflect true systemic bacteremia. Furthermore, drawing cultures clustered close together fails to demonstrate the continuous, sustained nature of the intravascular infection.
3.Administering the first dose of prescribed broad-spectrum antibiotics before drawing culturesis a critical procedural error that causes false negatives. Even a single dose of an antimicrobial agent can rapidly suppress bacterial growth in the culture bottle, masking the identity of the true pathogen. Antibiotics must be strictly withheld until after all culture sets are completed to preserve microbiological diagnostic yield.
4.Delaying cultures until the child's temperature spikes above 38.5oC is unnecessary and inappropriately postpones essential medical therapy. Unlike localized abscesses that release bacteria intermittently during chills, endocardial vegetations shed microbes into the bloodstream continuously. Because bacteremia is constant, blood cultures can be successfully drawn at any time regardless of fluctuating fever patterns.
Test-taking strategy:
- Analyze the scenario/question: The nurse is preparing to collect blood cultures for a child suspected of having infective endocarditis. The nurse must select the action that ensures maximum diagnostic accuracy.
- Apply microbiological principles:
- Choice 2is correct because endocarditis guidelines mandate pulling multiple distinct peripheral samples over time to verify persistent, continuous bacteremia and rule out skin contaminants.
- Identify timing pitfalls:
- Rule out Choice 3because administering antibiotics prior to cultures sterilizes the blood sample, preventing the lab from identifying the specific organism.
- Recognize pathophysiology:
- Rule out Choice 4because endocarditis causes continuous, not intermittent, bacteremia, making it obsolete to wait for a temperature spike.
- Evaluate contamination risks:
- Rule out Choice 1because indwelling central lines are prone to local contamination and pulling all samples at once defeats the purpose of proving sustained bacteremia.
Take home points:
- Diagnosing infective endocarditis requires drawing a minimum of three sets of blood cultures from separate peripheral venipuncture sites.
- Blood cultures must be completed prior to the initiation of any empirical antibiotic therapy to avoid suppressing microbial growth.
- Bacteremia in endocarditis is continuous rather than transient, meaning culture collection does not need to align with fever spikes.
- Central venous line ports are avoided for diagnostic cultures due to the high risk of misleading results from catheter biofilm colonization.
Practice Excercise 1
A 17-year-old client has acute infective endocarditis. While obtaining a nursing history, what should the nurse ask the client about? Select all that apply
Explanation
When gathering a nursing history for a client with acute infective endocarditis,the nurse focuses on identifying activities, behaviors, or recent infections that breach the body's natural barriers.Acute endocarditis is highly aggressive, typically driven by virulent pathogens like Staphylococcus aureus, which require rapid identification of the primary portal of entry.
Rationale for correct answers:
2.IV drug abuseis a primary risk factor for acute infective endocarditis, particularly in adolescents and young adults. Injecting non-sterile substances with contaminated needles introduces pathogens directly into the venous system. These bacteria travel to the right side of the heart, frequently attacking the tricuspid valve, leading to rapid valvular destruction and septic pulmonary embolization.
3.Recent dental workinvolving manipulation of the gingival tissue or perforation of the oral mucosa causes transient bacteremia. Normal oral flora, especially Viridans group streptococci, enter the bloodstream through these mucosal breaks and can rapidly colonize vulnerable endocardial surfaces.
5.A recent urinary tract infection (UTI)or associated urological manipulation can introduce pathogens like Enterococcusspecies or Gram-negative bacilli into the circulation. Translocation of bacteria from an untreated localized infection into the bloodstream is a well-documented pathway for cardiac seeding.
Rationale for incorrect answers:
1.An appendectomyis an intra-abdominal surgical procedure. If performed under standard sterile conditions in the past, it does not pose an ongoing risk for acute infective endocarditis. Unless the surgery was complicated by active, untreated systemic sepsis immediately preceding the cardiac symptoms, it is irrelevant to the current assessment.
4.Cardiac catheterizationis a sterile percutaneous diagnostic procedure. While any vascular entry carries a theoretical risk, the incidence of endocarditis following a standard diagnostic catheterization is exceptionally low compared to indwelling central lines, implantable devices, or active intravenous drug use, making it a lower priority during history gathering.
Test-taking strategy:
- Analyze the Scenario:A 17-year-old has acute infective endocarditis. The goal is to select historical factors that act as portals of entry or high-yield risk factors for blood streaming infections.
- Identify portals of entry:
- Choices 2 and 3are classic, high-yield historical triggers across all boards because they represent immediate disruptions to the skin or mucosal barriers.
- Choice 5represents an active infectious reservoir capable of seeding the bloodstream.
- Eliminate low-risk sterile procedures:
- Eliminate Choice 1and Choice 4because sterile, uncomplicated procedures (especially a routine abdominal surgery like an appendectomy) do not provide a standard mechanism for acute bacterial endocardial colonization.
Take-Home Points
- Acute infective endocarditis is a medical emergency characterized by rapid, destructive vegetative growth on cardiac valves, most commonly from Staphylococcus aureus.
- History-taking must aggressively investigate any recent skin breaches (IV drug use, tattoos, body piercings) and mucosal disruptions (dental interventions).
- Right-sided endocarditis (tricuspid valve) is heavily associated with intravenous drug use and presents with septic pulmonary complications.
A 14-year-old adolescent with a history of intravenous drug use is admitted with suspected right-sided infective endocarditis. The nurse knows that which valve is most commonly affected in this population?
Explanation
Right-sided infective endocarditisin intravenous drug users primarily results from the direct inoculation of skin flora into the venous system. It presents with septic pulmonary emboli,persistent bacteremia, and a holosystolic murmur that intensifies during inspiration.
Rationale for correct answer:
3.The tricuspid valveis the most frequently involved site, accounting for over 75% of cases in this population. Microscopic endothelial trauma from injected particulate matter creates a nidus for bacterial adherence. Staphylococcus aureusis the predominant pathogen isolated.
Rationale for incorrect answers:
1.The mitral valveis the most common site for left-sided infective endocarditis in the general population, but it is less frequently affected initially in individuals who practice intravenous drug use. Left-sided involvement carries a much higher risk of systemic arterial embolization.
2.The aortic valveis another left-sided structure that is typically affected by congenital defects, degenerative disease, or rheumatic heart disease. While it can be involved in intravenous drug users, it is statistically less common than right-sided tricuspid infection.
4.The pulmonic valveis rarely affected in isolation during infective endocarditis, even within the intravenous drug-using population. When right-sided endocarditis occurs, it almost exclusively targets the tricuspid valve before any potential secondary involvement of the pulmonary valvular apparatus.
Test-taking strategy:
- Analyze the scenario/question: The patient is a 14-year-old intravenous drug user with suspected right-sided infective endocarditis. The nurse must identify the anatomical valve most vulnerable to infection within this specific high-risk demographic group.
- Evaluate pathophysiology:
- Intravenous drug use introduces pathogens directly into the peripheral venous circulation, meaning the bacteria travel through the vena cava and hit the right side of the heart first.
- Rule in Choice 3because the tricuspid valve is the first cardiac valve encountered by venous blood flow coming from the systemic circulation.
- Identify anatomical locations:
- Rule out Choice 1and Choice 2because the mitral and aortic valves are left-sided structures, which are typically seeded either via the arterial system or secondary to left-to-right shunts.
- Rule out Choice 4because the pulmonic valve has a lower incidence of vegetation formation compared to the tricuspid valve, despite being on the right side.
Take home points
- The tricuspid valve is the most common site of infective endocarditis in intravenous drug users due to the direct path of contaminated venous blood.
- Staphylococcus aureus is the most frequent causative organism in right-sided infective endocarditis associated with intravenous drug use.
- Clinical manifestations often include respiratory symptoms caused by septic pulmonary emboli rather than systemic embolic events.
- Diagnostic confirmation requires positive blood cultures and echocardiographic evidence of valvular vegetations or myocardial abscesses.
The nurse is conducting a staff education program on infective endocarditis. During the pathophysiological development of infective endocarditis, what directly protects the proliferating microcolonies of bacteria from the host's immune response?
Explanation
Infective endocarditisdevelops when damaged valvular endothelium triggers a localized coagulation cascade, leading to a sterile thrombus.Circulating pathogens adhere to this matrix, proliferating into dense microcolonies that induce continuous fibrin-platelet deposition,creating an avascular vegetation that shields bacteria from phagocytic clearanceand limits antibiotic penetration.
Rationale for correct answer:
2.The fibrin-platelet matrixcontinuously deposits over the proliferating bacteria, acting as a physical barrier. This protective coatingprevents neutrophils and complement proteins from reaching the pathogens, facilitating unchecked microbial replication within the vegetation.
Rationale for incorrect answers:
1.The bacterial capsuleis composed of polysaccharides or polypeptides rather than adipose tissue. While capsules contribute to immune evasion by inhibiting opsonization, the structural protection within endocarditis vegetations is derived from host-derived coagulation factors, not bacterial fat layers.
3.The bacterial exotoxinsmay damage host cells, but rapid destruction of leukocytes is not the primary mechanism of protection. The microcolonies survive because the avascular, dense structure of the vegetation physically prevents immune cells from infiltrating the site of infection.
4.The myocardial infiltrationcan occur as a complication, such as a perivalvular abscess, but it is not the mechanism protecting microcolonies. The primary pathology remains localized to the endocardial surface leaflets where the avascular fibrin meshwork provides a sanctuary.
Test-taking strategy:
- Analyze the scenario/question: The nurse is educating staff on the pathophysiology of infective endocarditis. The question asks for the specific mechanism that directly shields proliferating bacterial microcolonies from the host immune defenses.
- Evaluate pathophysiology:
- The hallmark of infective endocarditis is the formation of a vegetation, which is a mix of pathogens, platelets, and clotting factors.
- Rule in Choice 2because the continuous layer of host clotting factors creates a physical sanctuary that isolates bacteria from circulating immune components.
- Identify inaccuracies:
- Rule out Choice 1because cardiac vegetations and bacterial defenses do not utilize dense adipose tissue for protective barriers.
- Rule out Choice 3because while leukocidins exist, the mechanical barrier of the vegetation is the defining protective feature in endocarditis.
- Rule out Choice 4because endocarditis is primarily a disease of the endocardium and valves, not an initial deep myocardial invasion.
Take home points
- The formation of nonbacterial thrombotic endocarditis provides the initial adherence site for circulating pathogens during transient bacteremia.
- Aggregation of host fibrin and platelets covers the adherent bacteria, forming a mechanical barrier against phagocytosis.
- The avascular nature of cardiac valvular vegetations limits both host immune cell entry and the delivery of therapeutic antibiotic concentrations.
- Persistent growth within this protected matrix leads to structural valvular destruction and increases the risk of septic embolization.
The nurse is explaining the development of vegetations to a parent whose child has infective endocarditis. Which sequence best describes the pathophysiological formation of these lesions?
Explanation
Infective endocarditis vegetationpathogenesis requires disrupted valvular tissue. Endothelial injurytriggers localized deposition of fibrin and platelets, creating a sterile nidus where circulating microbes achieve bacterial adherence,driving progressive vegetation growth.
Rationale for correct answer:
2.The sequence accurately reflects the biological timeline. Endothelial injurymust occur first to expose the extracellular matrix. This initiates host clotting factor recruitment, creating a sterile meshwork that facilitates microbial attachmentduring bacteremia. This culminates in mature lesions.
Rationale for incorrect answers:
1.This sequence is incorrect because bacterial colonizationcannot happen before endothelial damage. Pathogens require a pre-existing platelet-fibrin matrix to adhere to the valvular surface. Without initial mechanical trauma, circulating bacteria cannot easily colonize healthy endocardial tissue.
3.This sequence is flawed because clotting cascadeactivation occurs as a direct consequence of endothelial disruption. Blood coagulation factors do not randomly aggregate on pristine valves without preceding tissue injury. Furthermore, colonization precedes the secondary layer of fibrin deposition.
4.This sequence inaccurately depicts the initial phase of vegetation development. Bacterial adherenceis a secondary phenomenon that relies entirely on a pre-formed sterile thrombus. Endothelial injury is the initiating event, not a late consequence of tissue necrosis.
Test-taking strategy:
- Analyze the scenario/question: The nurse is explaining vegetation development to a parent. The question requires selecting the correct chronological orderof pathophysiological events leading to vegetation formation.
- Evaluate chronological milestones:
- Cardiac damage always serves as the mandatory initiating factorin this cascade.
- Rule in Choice 2because it correctly identifies tissue traumafollowed by sterile thrombus formation before microbial seeding occurs.
- Identify sequential flaws:
- Rule out Choice 1because bacteria cannot colonize intact, healthy endocardium effectively without prior injury.
- Rule out Choice 3because coagulation pathwaysrequire exposure of subendothelial collagen to activate.
- Rule out Choice 4because attachment is impossible without the initial landing pad created by mechanical stress.
Take home points
- Endothelial damage from turbulent blood flow is the prerequisite step in vegetation formation.
- Platelets and fibrin aggregate at the injury site to form a sterile nonbacterial thrombotic endocarditis lesion.
- Circulating bacteria attach to this sterile matrix during episodes of transient bacteremia.
- Proliferating pathogens stimulate further fibrin deposition, sealing themselves inside an avascular protective cover.
An infant with a complex cyanotic congenital heart defect is admitted to the pediatric unit. The nurse identifies which factors as increasing this infant's risk for infective endocarditis? Select all that apply
Explanation
Infective endocarditissusceptibility in cyanotic congenital heart disease peaks due to compromised hemodynamics and invasive access. Vulnerability escalates via endothelial shear stress, presence of prosthetic materials, and intravenous cannulation, facilitating microbial colonization over damaged cardiac structures.
Rationale for correct answers:
1.The systemic-to-pulmonary shuntintroduces prosthetic material and turbulent flow, creating an optimal substrate for bacterial adherence. These synthetic conduits experience high velocity gradients that strip endothelium and encourage platelet aggregation.
2.The PICC linebreaches epithelial defensesand provides direct venous access to the heart. Indwelling central catheters can mechanically traumatize right-sided endocardial tissue, forming a sterile nidus for circulating pathogens.
5.The endothelial traumafrom high-velocity blood jettingthrough complex structural defects continuously exposes subendothelial collagen. This mechanical wear initiates the localized clotting cascade necessary for vegetation development.
Rationale for incorrect answers:
3.The secondary polycythemiadriven by chronic hypoxia increases blood viscosity and risk of thrombosis, but it does not directly shield or predispose the endocardium to microbial seeding. Hyperviscosity affects microvascular perfusion rather than valvular endothelial integrity.
4.The diaper changescause localized skin friction but do not induce transient bacteremia. While mucosal disruption from dental or surgical interventions seeds pathogens, routine hygiene care does not introduce bacteria into the systemic bloodstream.
Test-taking strategy:
- Analyze the scenario/question: The patient is an infant with a complex cyanotic congenital heart defect. The nurse must select all risk factors that actively increase the likelihood of developing infective endocarditis.
- Evaluate pathophysiologic risk factors:
- Rule in Choice 1because artificial shunts create turbulent flow and introduce foreign materials that lack host immune defenses.
- Rule in Choice 2because central venous catheters violate vascular integrity and can physically irritate cardiac endocardium.
- Rule in Choice 5because high-velocity jets are the classic driver of structural endothelial denudation.
- Eliminate non-contributory factors:
- Rule out Choice 3because while elevated hematocrit is common in cyanotic defects, it is a hematologic compensation, not an endocarditis driver.
- Rule out Choice 4because regular external cleansing does not breach deep mucosal barriers to cause systemic bacteremia.
Take home points
- Cyanotic congenital heart defects combined with prosthetic shunts carry the highest category of endocarditis risk.
- Central venous access devices present a dual threat by breaching skin barriers and causing direct mechanical endocardial irritation.
- High-velocity turbulent blood flow through unrepaired septal defects or stenotic valves drives the prerequisite endothelial injury.
- Prophylactic antibiotic protocols are strictly indicated for high-risk cardiac patients prior to specific invasive mucosal procedures.
The nurse is assessing a child with a history of rheumatic heart disease. The nurse understands that this condition predisposes the child to infective endocarditis primarily due to which factor?
Explanation
Rheumatic heart diseasepredisposes individuals to infective endocarditisthrough autoimmune-mediated structural damage to cardiac architecture. Chronic inflammation causes valvular fibrosis,resulting in thickened leafletsand surface irregularities that create a permanent nidus for mechanical turbulence and subsequent platelet-fibrin depositionduring episodes of bacteremia.
Rationale for correct answer:
2.The valvular scarringand structural deformation permanently alter normal laminar blood flow, creating severe turbulence. This mechanical stress strips the endothelial lining, exposing subendothelial collagen and initiating the localized clotting cascade that serves as a docking site for circulating bacteria.
Rationale for incorrect answers:
1.The immune suppressionis not a primary pathological feature of rheumatic heart disease. Rheumatic fever is characterized by a hypersensitivity autoimmune response rather than an immunodeficiency state, meaning the host immune system is overactive rather than chronically suppressed.
3.A genetic mutationaltering endothelial receptor binding is not the mechanism driving endocarditis risk in this population. The predisposition is entirely acquired through structural tissue damage from prior molecular mimicry between group A streptococcal antigens and human endocardial tissue.
4.The erythrocyte overproductionleading to microvascular occlusion is characteristic of cyanotic congenital heart conditions causing chronic hypoxia, not rheumatic heart disease. Valvular deformities alter macrovascular cardiac hemodynamics rather than inducing secondary polycythemia or clogging the capillary bed.
Test-taking strategy:
- Analyze the scenario/question: The patient has a history of rheumatic heart disease. The nurse needs to identify the primary pathophysiological factor that connects this specific past medical condition to an increased risk of developing infective endocarditis.
- Evaluate structural changes:
- Rheumatic fever inflicts structural, mechanical injuries on the cardiac skeleton, particularly targeting the mitral and aortic valvular apparatus.
- Rule in Choice 2because permanent fibrotic changes and leaflet thickening provide the exact rough surface needed for fibrin-platelet thrombi to form.
- Differentiate pathologies:
- Rule out Choice 1because rheumatic disease is an autoimmune inflammatory condition, not an immunodeficiency state.
- Rule out Choice 3because the disease process is acquired via post-streptococcal autoimmunity, not an inherited endothelial genetic mutation.
- Rule out Choice 4because altered blood viscosity and secondary polycythemia are associated with cyanotic lung or heart defects, not rheumatic valvulitis.
Take home points
- Rheumatic heart disease damages valves via molecular mimicry following an untreated group A beta-hemolytic streptococcal pharyngitis infection.
- Chronic valvular scarring and thickening lead to stenotic or regurgitant lesions that generate high-velocity turbulent jet streams.
- Exposed subendothelial collagen on damaged rheumatic leaflets triggers the formation of nonbacterial thrombotic endocarditis lesions.
- These pre-existing sterile thrombi readily trap circulating bacteria during routine daily activities or invasive dental procedures.
The nurse is teaching a student nurse about the hemodynamic factors that contribute to IE. The nurse explains that vegetations most commonly form in areas where blood flows from:
Explanation
Infective endocarditis vegetationsdevelop predominantly under specific hemodynamic gradients where high-velocity flow causes mechanical stress. Blood jetting from a high-pressure zonethrough a narrow orificeinto a low-pressure zoneinduces severe endothelial shear injury, creating an avascular sink downstream where platelet-fibrin thrombisettle and trap circulating pathogens.
Rationale for correct answer:
2.The venturi effectcreated by high-velocity flowthrough a restricted opening causes a drop in lateral pressure immediately downstream in the low-pressure chamber. This pressure drop minimizes endothelial shear at that exact site, allowing bacteria and platelets to deposit and form a stable vegetation.
Rationale for incorrect answers:
1.A flow from a low-pressure areainto a high-pressure area is thermodynamically impossible without an active mechanical pump moving against the hydrostatic gradient. Fluid dynamics dictate that blood naturally moves down its pressure gradient, moving from higher to lower pressure zones during cardiac cycles.
3.Two equal pressure chambersdo not generate the high-velocity turbulent jets required to strip the endothelial lining of cardiac structures. Without a significant pressure differential, laminar blood flow is preserved, which prevents the mechanical trauma necessary to expose subendothelial collagen.
4.The peripheral venulesreceive blood from indwelling lines, but this describes a route of bacterial inoculation rather than a hemodynamic mechanism driving intracardiac vegetation localization. Valvular vegetations require specific intracardiac pressure differentials that are entirely absent within low-velocity peripheral venous architecture.
Test-taking strategy:
- Analyze the scenario/question: The nurse is instructing a student nurse on the fluid dynamics and hemodynamic factors that dictate where infective endocarditis vegetations typically develop inside the heart.
- Apply principles of fluid dynamics:
- Vegetations form according to Rodbard's principles, which state that lesions develop immediately downstream from a narrow orifice where blood transitions from high to low pressure.
- Rule in Choice 2because a high-to-low pressure drop through a narrow opening (like a stenotic valve or septal defect) creates the turbulent downstream eddy where thrombi precipitate.
- Eliminate illogical options:
- Rule out Choice 1because fluid cannot spontaneously flow backwards from a low-pressure zone into a high-pressure zone.
- Rule out Choice 3because equal pressures maintain quiet, non-turbulent flow, which lacks the mechanical force to cause endothelial injury.
- Rule out Choice 4because while IV lines provide an entry portal for microbes, they do not represent the intracardiac hemodynamic gradients that dictate structural vegetation placement.
Take home points
- Intracardiac vegetations characteristically form on the low-pressure side of a structural cardiac defect or abnormal valve leaflet.
- High-velocity jet streams traveling through narrow orifices cause significant endothelial erosion at the impact site.
- The pressure drop immediately past a narrow opening creates localized eddies that favor the precipitation of fibrin, platelets, and bacteria.
- Typical examples include the atrial surface of incompetent AV valves and the ventricular surface of a ventricular septal defect.
The nurse is teaching parents about how transient bacteremia leads to infective endocarditis. Which everyday activities or events can introduce bacteria into the bloodstream of a child with a predisposing heart condition? Select all that apply
Explanation
Transient bacteremiaoccurs when physical manipulation of mucosal surfaces allows normal flora to breach epithelial barriers and enter the circulatory system. In children with high-risk cardiac lesions, mucosal traumafrom routine activities or professional procedures can seed bacteria, facilitating microbial disseminationand colonization of pre-existing valvular thrombi.
Rationale for correct answers:
1.The vigorous brushingof compromised, inflamed gingival tissue disrupts friable mucosal capillaries, allowing oral commensals like Streptococcus viridansto directly enter the venous bloodstream. The frequency of these repetitive daily exposures significantly compounds the cumulative risk of endocardial seeding.
3.A dental cleaninginvolves mechanical instrumentation of the subgingival space, which routinely causes transient bacteremia. Scaling and root planing break epithelial bonds around the teeth, providing an immediate portal of entry for oral microbes into the systemic circulation.
4.The act of chewing foodwhen periodontal disease is activeforces oral bacteria through compromised periodontal pockets via masticatory pressure. Severe inflammation lowers the mechanical threshold required for mucosal barrier failure, enabling transient bacteremia during regular meals.
Rationale for incorrect answers:
2.The skin cleansingof healthy, intact epithelium does not breach vascular barriers or introduce pathogens into the bloodstream. Antimicrobial soap removes superficial skin flora but lacks the mechanical or invasive capacity to disrupt deep subdermal tissue or venous capillaries.
5.The public poolswimming exposes the skin to chlorinated water but does not cause transient bacteremia. Because chlorine neutralizes most waterborne pathogens and intact skin serves as an impenetrable barrier, recreational swimming does not introduce microorganisms into the systemic vascular system.
Test-taking strategy:
- Analyze the scenario/question: The nurse is educating parents on how transient bacteremia triggers infective endocarditis. The question requires selecting all daily activities or events that can introduce bacteria into a child's blood circulation.
- Evaluate mucosal integrity:
- Rule in Choice 1because mechanical friction against inflamed, vascular gums breaks the epithelial lining and allows oral flora to enter capillaries.
- Rule in Choice 3because professional subgingival manipulation breaks tissue barriers and is a classic, high-risk cause of bacteremia.
- Rule in Choice 4because mastication on diseased periodontal tissues exerts substantial pressure that pushes resident bacteria into disrupted blood vessels.
- Eliminate intact external barriers:
- Rule out Choice 2because washing skin does not damage blood vessels or breach dermal defenses.
- Rule out Choice 5because submersion in chlorinated water does not violate mucous membranes or open a path into the venous system.
Take home points
- Transient bacteremia is most frequently caused by daily activities involving mucosal friction rather than isolated medical events.
- Chronic oral inflammation and periodontal disease lower the structural threshold for bacteria to cross into the bloodstream.
- Viridans group streptococci are the primary oral pathogens introduced into circulation during dental manipulation or hygiene activities.
- Maintaining optimal routine oral health is the most critical preventive strategy to reduce the frequency and intensity of spontaneous bacteremia.
The nurse cares for a child with a large ventricular septal defect (VSD). The nurse notes that the vegetations of infective endocarditis are located on the right ventricular side of the defect wall. The nurse attributes this to which hemodynamic principle?
Explanation
Infective endocarditis vegetation localizationis governed by the structural consequences of high-velocity fluid dynamics across cardiac pressure gradients. Blood shunting through a restrictive ventricular septal defect creates a powerful systolic jet streamthat inflicts mechanical endothelial shear injurydownstream against the lower-pressure right ventricular wall, triggering the platelet-fibrin depositionthat serves as a docking site for circulating bacteria.
Rationale for correct answer:
3.The venturi effectdictates that blood moving from the high-pressure left ventriclethrough a restrictive defect accelerates into a high-velocity jet. As this stream enters the lower-pressure right ventricle, it strikes the opposing endocardium, denuding endothelial cells and exposing subendothelial collagen.
Rationale for incorrect answers:
1.The oxygen concentrationwithin cardiac chambers does not dictate where bacteria adhere or proliferate during infective endocarditis. While some pathogens are obligate or facultative, the primary determinants of vegetation localization are mechanical tissue trauma and altered blood flow velocity, not localized partial pressures of oxygen.
2.The bacterial loaddoes not physically precipitate or drop out of solution as blood traverses a septal defect. Bacteria remain uniformly suspended within circulating plasma; they only drop out and colonize a specific anatomical site when trapped by a pre-formed, sticky meshwork of host platelets and clotting factors.
4.The right ventricularpressures are naturally much lower than left ventricular pressures in a normal heart or one with a restrictive left-to-right shunt. High-pressure zones do not force bacteria to stick; rather, the mechanical impact of blood flowing into a lower-pressure zone creates the downstream turbulence that fosters vegetation growth.
Test-taking strategy:
- Analyze the scenario/question: The nurse is caring for a child with a large ventricular septal defect and notes that vegetations are located on the right ventricular side of the shunt. The question requires identifying the hemodynamic principle that explains this specific localization.
- Apply principles of cardiovascular dynamics:
- Blood naturally shunts from a zone of high pressure (left ventricle) to a zone of lower pressure (right ventricle).
- Rule in Choice 3because the high-velocity stream crossing the septum hits the right ventricular endocardium, creating a localized patch of mechanical tissue injury.
- Eliminate inaccurate assumptions:
- Rule out Choice 1because metabolic gas gradients do not guide the mechanical adhesion of bacteria to cardiac tissue.
- Rule out Choice 2because blood does not filter or shed its microbiological content during transit across a structural defect.
- Rule out Choice 4because it incorrectly reverses normal cardiac physiology, as left ventricular pressure exceeds right ventricular pressure.
Take home points
- Intracardiac vegetations form downstream from a restrictive defect where a high-velocity jet transitions into a lower-pressure chamber.
- The mechanical impact of a left-to-right shunt jet erodes the endocardium of the receiving chamber wall.
- Endothelial denudation at the impact site initiates localized clotting factor assembly and platelet aggregation.
- The resulting sterile nonbacterial thrombus traps circulating microbes during episodes of transient bacteremia.
The nurse is teaching a group of nursing students about the turbulent blood flow theory in the pathophysiology of pediatric infective endocarditis. Which structural factors should the nurse include as primary drivers of this turbulent flow? Select all that apply
Explanation
Pediatric infective endocarditisrelies heavily on fluid dynamics that disrupt normal laminar blood flow. Turbulent blood flowoccurs when significant pressure differentials force fluid across restricted openings, generating high shear stressthat causes endothelial denudation, which serves as a mandatory landing pad for circulating microorganisms.
Rationale for correct answers:
1.The high-velocity streamsrushing through a constricted opening create extreme mechanical friction against adjacent cardiac walls. This concentrated kinetic energy disrupts orderly blood flow, generating downstream eddies and shear forces that tear the protective endothelial cell lining.
3.The pressure differentialbetween a high-pressure chamber and a low-pressure chamber drives rapid acceleration of blood across the dividing barrier. This extreme velocity gradient destabilizes laminar flow, producing the turbulent impact zones required to initiate a sterile platelet-fibrin thrombus.
Rationale for incorrect answers:
2.The systemic hypotensionreduces blood flow velocity and driving pressures throughout the cardiovascular system. Lowering the kinetic energy of blood flow minimizes rather than accelerates the mechanical turbulence and shear forces that cause endocardial tissue damage.
4.The atrial septaldefect involves large structural openings with very low pressure gradients between the left and right atria. Blood moves across this defect quietly and slowly, preserving non-turbulent laminar flow patterns that fail to cause mechanical endothelial erosion.
5.The catheter traumarepresents a mechanical, physical violation of the endothelial wall by a foreign body rather than a hemodynamic driver of turbulent blood flow. While indwelling lines cause injury, they do so through direct contact friction rather than fluid-driven shear forces.
Test-taking strategy:
- Analyze the scenario/question: The nurse is instructing students on the turbulent blood flow theory in pediatric infective endocarditis. The question requires selecting all structural factors that actively drive mechanical fluid turbulence.
- Apply fluid dynamic principles:
- Turbulence requires high kinetic energy, velocity changes, and abrupt transitions across sharp pressure gradients.
- Rule in Choice 1because narrowing an orifice accelerates fluid into a high-velocity jet stream, which breaks up orderly flow.
- Rule in Choice 3because a steep pressure drop between chambers is the primary engine that drives rapid, turbulent fluid acceleration.
- Eliminate low-energy and non-fluid drivers:
- Rule out Choice 2because low blood pressure dampens fluid velocities and decreases mechanical shear stress.
- Rule out Choice 4because low-pressure, large-diameter openings produce slow, smooth shunting without downstream impact zones.
- Rule out Choice 5because catheter-induced injury is a direct mechanical scratching of the wall, not a fluid-driven turbulence phenomenon.
Take home points
- Turbulent blood flow theory dictates that mechanical fluid forces are the primary initiators of the prerequisite endocardial lesion.
- High-velocity jets moving through tight openings cause a severe drop in lateral pressure immediately past the constriction.
- This drop in pressure allows host clotting elements to precipitate out of the turbulent eddies and settle on the downstream wall.
- Structural defects with minimal pressure gradients carry a significantly lower statistical risk of developing infective endocarditis.
Practice Excercise 2
A 7-year-old child is diagnosed with acute infective endocarditis caused by Staphylococcus aureus. The nurse recognizes that this form of the disease differs from subacute endocarditis because it is characterized by:
Explanation
Acute infective endocarditis caused by Staphylococcus aureusis a fulminant systemic infection characterized by rapid disease progression. Unlike subacute variants, it features valvular destruction, intense systemic toxicity, high-grade bacteremia, and a pronounced tendency for metastatic abscessformation across multiple organ systems.
Rationale for correct answer
2.The fulminant progressiondriven by Staphylococcus aureusresults from its high virulence and expression of destructive exoenzymes. It causes rapid, necrotizing destruction of cardiac tissues within days, leading to acute valvular incompetence, mechanical heart failure, and profound sepsis.
Rationale for incorrect answers
1.A slow, insidiousonset over several weeks or months is the hallmark of subacute infective endocarditis, typically caused by low-virulence organisms like Streptococcus viridans. Acute endocarditis presents abruptly with high spiking fevers and rapid clinical deterioration over a few days.
3.The unaffected heartscan certainly be targeted by Staphylococcus aureusdue to its ability to adhere to normal endothelial cells, but it does not exclusively affect children without defects. It readily infects both structurally abnormal and healthy cardiac anatomy.
4.The embolic riskis exceptionally high in acute Staphylococcus aureusendocarditis, not minimal. The vegetations formed by this pathogen are highly friable, rapidly growing, and prone to breaking off, causing widespread septic embolization to the brain, kidneys, and lungs.
Test-taking strategy:
- Analyze the scenario/question: A 7-year-old is diagnosed with acute infective endocarditis caused by Staphylococcus aureus. The nurse must identify the clinical characteristic that differentiates this acute form from subacute endocarditis.
- Contrast Virulence and Progression:
- Acute endocarditis implies a high-velocity, highly destructive clinical course driven by an aggressive, pyogenic pathogen.
- Rule in Choice 2because Staphylococcus aureusrapidly destroys valvular leaflets and causes severe, toxic systemic manifestations.
- Eliminate Subacute Characteristics:
- Rule out Choice 1because an insidious, prolonged timeline describes subacute infections caused by less aggressive bacteria.
- Rule out Choice 3because while it can attack normal valves, the word "exclusively" is a modifier that invalidates the choice since it also attacks malformed valves.
- Rule out Choice 4because larger, highly friable staphylococcal vegetations dramatically increase the threat of embolic strokes and systemic infarcts.
Take home points
- Acute infective endocarditis is a medical emergency characterized by rapid clinical deterioration and overwhelming bacterial sepsis.
- Staphylococcus aureus produces aggressive toxins and proteases that cause rapid tissue necrosis and valvular perforation.
- Subacute endocarditis is more commonly associated with low-virulence oral commensals and follows a indolent course.
- Complications of the acute form frequently include early-onset congestive heart failure and multiple septic emboli.
The nurse is caring for a teenager with suspected infective endocarditis. According to the Modified Duke Criteria, which of the following findings is categorized as a major criterion for diagnosing infective endocarditis?
Explanation
The diagnosis of infective endocarditis relies on the Modified Duke Criteria, which stratify clinical findings into major and minor categories. Diagnostic confirmation requires objective evidence of endocardial involvement, specifically echocardiographic visualizationof vegetations, or the isolation of typical pathogens from serial blood cultures, whereas systemic vascular and immunologic phenomena serve as minor criteria.
Rationale for correct answer
3.The oscillating intracardiac massdetected via echocardiography provides definitive structural evidence of endocardial involvement, satisfying a major diagnostic criterion. Imaging must demonstrate a vegetation, abscess, or new partial dehiscence of a prosthetic valve to fulfill this specific high-weight parameter.
Rationale for incorrect answers
1.A pyrexial spikeexceeding 38.0 degrees Celsius satisfies a minor diagnostic criterion under the clinical categories, not a major one. Fever is a highly sensitive but non-specific systemic inflammatory response that occurs in numerous pediatric infectious and autoimmune conditions.
2.The Roth spotsrepresent an immunologic phenomenon resulting from immune complex deposition in the retinal microvasculature, which is classified strictly as a minor criterion. Other immunologic findings in this category include glomerulonephritis, Osler nodes, and a positive rheumatoid factor.
4.The microscopic hematuriais a secondary clinical sign that often stems from embolic renal infarction or immune-mediated glomerulonephritis, classifying it as a minor criterion. It lacks the diagnostic specificity required to establish primary endocardial infection in isolation.
Test-taking strategy:
- Analyze the scenario/question: The nurse is evaluating a teenage patient with suspected infective endocarditis. The question requires identifying which of the provided clinical or laboratory findings constitutes a major criterion according to the Modified Duke Criteria.
- Classify Diagnostic Parameters:
- The Modified Duke Criteria reserve major status for direct microbiologic isolation of classic pathogens or definitive structural cardiac imaging.
- Rule in Choice 3because an oscillating mass seen on an echocardiogram is the classic imaging hallmark of endocardial vegetation, fulfilling the major imaging criterion.
- Differentiate Minor Criteria:
- Rule out Choice 1because a core body temperature elevation is a general systemic sign categorized as a minor criterion.
- Rule out Choice 2because retinal micro-hemorrhages are immunologic manifestations, which are explicitly relegated to minor status.
- Rule out Choice 4because renal vascular or inflammatory shedding of blood cells is a secondary complication that falls under minor vascular or immunologic categories.
Take home points
- Pathological or clinical diagnosis via the Modified Duke Criteria requires two major, one major and three minor, or five minor criteria.
- The two primary major criteria are persistently positive blood cultures with typical organisms and echocardiographic evidence of endocardial injury.
- Vascular minor criteria include major arterial emboli, septic pulmonary infarcts, mycotic aneurysms, intracranial hemorrhages, and Janeway lesions.
- Immunologic minor criteria consist of glomerulonephritis, Osler nodes, Roth spots, and laboratory confirmation of an elevated rheumatoid factor.
The nurse is assessing an adolescent with suspected acute infective endocarditis. During a skin assessment, the nurse notes flat, painless, small red macules scattered across the palms of the patient's hands. The nurse should document these as:
Explanation
Peripheral cutaneous manifestations provide critical diagnostic clues for infective endocarditis, reflecting distinct underlying pathophysiological processes. Flat, painless macules on the palms or soles arise from microembolic vascular phenomena, whereas tender, raised nodules represent immunological deposition, requiring precise clinical differentiation to track systemic complications.
Rationale for correct answer
2.The Janeway lesionsare non-tender, erythematous macules that typically appear on the palms and soles. They are caused by septic microemboli dislodged from cardiac vegetations that occlude peripheral dermal capillaries, leading to localized microinfarctions and neutrophilic infiltration without an immune complex etiology.
Rationale for incorrect answers
1.The Osler nodesare painful, tender, raised nodules that characteristically develop on the pads of the fingers and toes. Unlike Janeway lesions, they are immunologic phenomena caused by the deposition of circulating immune complexes in the local cutaneous vasculature rather than direct septic microembolization.
3.The splinter hemorrhagespresent as linear, dark-red streaks running longitudinally beneath the nail beds. While they can occur in infective endocarditis due to microemboli or capillary damage, they are anatomically restricted to the subungual tissue and do not manifest as palmar macules.
4.The erythema marginatumis a characteristic migratory, non-pruritic, erythematous rash with elevated borders that appears primarily on the trunk and proximal extremities. It is a major Jones criterion for acute rheumatic fever, not a vascular or immunologic sign of infective endocarditis.
Test-taking strategy:
- Analyze the scenario/question: The nurse is evaluating an adolescent with suspected acute infective endocarditis and observes flat, painless, small red macules on the palms. The nurse must identify the correct clinical term and underlying mechanism.
- Differentiate Cutaneous Manifestations:
- Use the mnemonic "Janeway is painless, Osler is ouch" to quickly separate the two classic peripheral skin signs of endocarditis based on tenderness.
- Rule in Choice 2because Janeway lesions match the description of being flat, painless palmar macules driven by vascular emboli.
- Eliminate Incompatible Alternatives:
- Rule out Choice 1because Osler nodes are explicitly painful, raised nodules driven by immune complexes.
- Rule out Choice 3because subungual micro-bleed streaks are morphologically and anatomically distinct from broad palmar lesions.
- Rule out Choice 4because this marginated ring rash is linked to rheumatic fever cascades, not direct endocarditis microembolization.
Take home points
- Janeway lesions are painless, erythematous macules on the palms and soles caused by septic microemboli from cardiac vegetations.
- Osler nodes are painful, raised nodules on the distal digits caused by localized immune complex deposition.
- Meticulous daily skin and nail bed assessments are crucial for detecting peripheral vascular and immunologic signs of endocarditis progression.
- Peripheral cutaneous signs are categorized as minor criteria under the Modified Duke Criteria for diagnosing infective endocarditis.
The nurse is assessing a 10-year-old child with suspected infective endocarditis. The nurse checks the child’s fingers and notes small, painful, intradermal nodules on the pads of the fingers. The nurse documents these findings as:
Explanation
Peripheral cutaneous manifestations provide critical diagnostic clues for infective endocarditis, reflecting distinct underlying pathophysiological processes. Tender, raised nodules on the distal extremities represent immunological deposition, whereas flat, painless macules arise from microembolic vascular phenomena, requiring precise clinical differentiation to track systemic complications.
Rationale for correct answer
2.The Osler nodesare painful, tender, raised nodules that characteristically develop on the pads of the fingers and toes. They are immunologic phenomena caused by the deposition of circulating immune complexes in the local cutaneous vasculature, triggering an inflammatory reaction.
Rationale for incorrect answers
1.The Janeway lesionsare non-tender, flat, erythematous macules that typically appear on the palms and soles. Unlike Osler nodes, they are caused by septic microemboli dislodged from cardiac vegetations that occlude peripheral dermal capillaries, leading to localized microinfarctions.
3.The splinter hemorrhagespresent as linear, dark-red streaks running longitudinally beneath the nail beds. While they can occur in infective endocarditis due to microemboli or capillary damage, they are anatomically restricted to the subungual tissue and do not manifest as painful nodules.
4.The Roth spotsare ophthalmoscopically identified retinal hemorrhages with central clearing or white spots. They represent an immunologic phenomenon resulting from immune complex deposition in the retinal microvasculature, rather than a cutaneous or intradermal manifestation on the digits.
Test-taking strategy:
- Analyze the scenario/question: The nurse is assessing a 10-year-old child with suspected infective endocarditis and notes small, painful, intradermal nodules on the pads of the fingers. The nurse must identify the correct clinical term.
- Differentiate Cutaneous Manifestations:
- Use the mnemonic "Osler is ouch, Janeway is painless" to quickly separate the two classic peripheral skin signs of endocarditis based on tenderness.
- Rule in Choice 2because Osler nodes match the description of being painful, raised nodules on the distal digits driven by immune complexes.
- Eliminate Incompatible Alternatives:
- Rule out Choice 1because Janeway lesions are explicitly painless, flat macules driven by vascular emboli.
- Rule out Choice 3because subungual micro-bleed streaks are morphologically and anatomically distinct from discrete nodular finger lesions.
- Rule out Choice 4because these lesions are restricted to the retina and cannot be observed on the external skin of the fingers.
Take home points
- Osler nodes are painful, raised nodules on the distal digits caused by localized immune complex deposition.
- Janeway lesions are painless, erythematous macules on the palms and soles caused by septic microemboli from cardiac vegetations.
- Meticulous daily skin and nail bed assessments are crucial for detecting peripheral vascular and immunologic signs of endocarditis progression.
- Peripheral cutaneous signs are categorized as minor criteria under the Modified Duke Criteria for diagnosing infective endocarditis.
A child must meet which minimum threshold of Modified Duke Criteria combinations to secure a definitive diagnosis of infective endocarditis?
Explanation
The clinical diagnosis of infective endocarditis requires structured risk stratification using objective diagnostic benchmarks. According to the Modified Duke Criteria, securing a definitive diagnosis relies on specific diagnostic thresholds, specifically requiring either two major criteria, a combination of one major criterion and three minor criteria, or five minor criteriato confirm endocardial infection.
Rationale for correct answer
2.The diagnostic thresholdfor definite infective endocarditis is strictly defined by these quantitative pairings. Meeting two major criteria, or one major criterion alongside three minor criteria, provides sufficient sensitivity and specificity to confirm the diagnosis without requiring direct histopathological tissue confirmation.
Rationale for incorrect answers
1.A combination of one majorand one minor criterion is insufficient to secure a definitive diagnosis. This low clinical payload falls into the possible infective endocarditis category, which requires further diagnostic workup, such as serial echocardiography or additional blood sampling, to rule out alternative pathologies.
3.The presence of three minorcriteria exclusively fails to cross the diagnostic threshold for definite endocarditis. While three minor criteria satisfy the baseline definition for possible infective endocarditis, they cannot independently validate endocardial infection without an accompanying major criterion or two additional minor findings.
4.The pairing of four minorcriteria with an elevated inflammatory marker does not secure a definitive diagnosis. While an elevated C-reactive protein is an expected systemic marker, the scoring system requires five distinct minor criteria in the absence of a major criterion to establish a definite diagnosis.
Test-taking strategy:
- Analyze the scenario/question: The question asks for the minimum threshold of Modified Duke Criteria combinations needed to establish a definitive clinical diagnosis of infective endocarditis in a pediatric patient.
- Recall Scoring Rules:
- Definite infective endocarditis can be established clinically through three specific pathways: 2 major, 1 major + 3 minor, or 5 minor criteria.
- Rule in Choice 2because it correctly identifies the two primary, highest-weight clinical scoring combinations used to secure a diagnosis.
- Eliminate Inadequate Combinations:
- Rule out Choice 1because 1 major and 1 minor criterion only qualify as a possible diagnosis, which is too weak for confirmation.
- Rule out Choice 3because 3 minor criteria satisfy the baseline for possible endocarditis but do not reach definite diagnostic status.
- Rule out Choice 4because 4 minor criteria do not meet the minimum non-major threshold of 5, and general inflammatory markers are non-specific additions.
Take home points
- A definite clinical diagnosis of infective endocarditis can be confirmed by satisfying 2 major criteria, 1 major and 3 minor criteria, or 5 minor criteria.
- Possible infective endocarditis is defined as meeting 1 major and 1 minor criterion, or 3 minor criteria.
- Major criteria focus exclusively on positive blood cultures showing typical microbes and echocardiographic evidence of endocardial involvement.
- Minor criteria encompass predisposing heart conditions, persistent fever, vascular phenomena, immunologic markers, and suggestive microbiologic data.
The nurse conducts an ophthalmoscopic examination alongside the health care provider for a child with suspected infective endocarditis. Retinal hemorrhages with pale centers are observed. How does the nurse classify this manifestation?
Explanation
Peripheral ocular and cutaneous manifestations provide critical diagnostic clues for infective endocarditis, reflecting distinct underlying pathophysiological processes. Retinal hemorrhages with pale centers represent immunological depositionwithin the ocular microvasculature, whereas cutaneous lesions arise from either microembolic vascular phenomenaor localized immune-mediated inflammation, requiring precise clinical differentiation to track systemic complications.
Rationale for correct answer
4.The Roth spotsare oval, retinal hemorrhages with central clearing or pale spots seen during fundoscopy. They are immunologic phenomena caused by the deposition of circulating immune complexes in the retinal capillaries, leading to localized microvascular rupture and subsequent healing patterns.
Rationale for incorrect answers
1.The Janeway lesionsare non-tender, flat, erythematous macules that typically appear on the palms and soles. Unlike Roth spots, they are caused by septic microemboli dislodged from cardiac vegetations that occlude peripheral dermal capillaries, leading to localized microinfarctions.
2.The Osler nodesare painful, tender, raised nodules that characteristically develop on the pads of the fingers and toes. They are immunologic phenomena caused by the deposition of circulating immune complexes in the local cutaneous vasculature, triggering an inflammatory reaction.
3.The splinter hemorrhagespresent as linear, dark-red streaks running longitudinally beneath the nail beds. While they can occur in infective endocarditis due to microemboli or capillary damage, they are anatomically restricted to the subungual tissue and do not manifest as retinal abnormalities.
Test-taking strategy:
- Analyze the scenario/question: The nurse and provider observe retinal hemorrhages with pale centers during an ophthalmoscopic examination of a child with suspected infective endocarditis. The nurse must identify the correct clinical term.
- Identify Anatomical Locations:
- Restrict choices based on the specific organ system being examined; the question describes a finding exclusively localized to the retina.
- Rule in Choice 4because Roth spots match the description of being retinal hemorrhages with pale, white centers driven by immune complexes.
- Eliminate Incompatible Alternatives:
- Rule out Choice 1because Janeway lesions are flat, painless macules restricted to the skin of the palms and soles.
- Rule out Choice 2because Osler nodes are painful, raised nodules restricted to the skin of the distal digits.
- Rule out Choice 3because subungual micro-bleed streaks are anatomically restricted to the tissue beneath the fingernails or toenails.
Take home points
- Roth spots are retinal hemorrhages with pale or white centers caused by localized immune complex deposition in the ocular capillaries.
- Osler nodes are painful, raised nodules on the distal digits caused by localized immune complex deposition.
- Janeway lesions are painless, erythematous macules on the palms and soles caused by septic microemboli from cardiac vegetations.
- Ocular and peripheral cutaneous signs are categorized as minor criteria under the Modified Duke Criteria for diagnosing infective endocarditis.
An infant is brought to the clinic with fever, poor feeding, and increased irritability. The parents state the infant has a history of tetralogy of Fallot. Which assessment finding is most critical for the nurse to report immediately when suspecting infective endocarditis?
Explanation
Infective endocarditis in infants with structural cardiac defects can cause rapid mechanical destruction of valvular and septal architectures. A dramatic transformation in hemodynamics alters acoustic properties, manifesting as a new or changing murmur, which indicates progressive vegetation growth, valvular perforation, or chordae rupture, and demands immediate cardiothoracic evaluationto avert mechanical heart failure.
Rationale for correct answer
1.A changing murmursignifies structural alteration of the cardiac valves or shunt margins due to expanding vegetations or tissue erosion. In an infant with tetralogy of Fallot, any acute alteration in the baseline murmur is a critical indicator of valvular incompetence or worsening outflow obstruction.
Rationale for incorrect answers
2.A diaper rashrepresents a localized, superficial dermal inflammation within the perineal skin folds, common in infants due to moisture and chemical irritation. While it requires appropriate topical nursing interventions, it is an expected skin variation and does not indicate systemic cardiac decompensation.
3.A weight lossof 2 ounces is a concerning sign of nutritional or metabolic stress in an infant, often secondary to the poor feeding associated with systemic infection. However, it does not represent an immediate, life-threatening structural cardiac emergency like acute valvular destruction.
4.The postprandial somnolenceor sleepiness after feedings can reflect generalized fatigue or increased work of breathing due to baseline hypoxemia in tetralogy of Fallot. Although it warrants monitoring, it is a non-specific behavioral finding rather than an acute indicator of architectural valvular damage.
Test-taking strategy:
- Analyze the scenario/question: An infant with tetralogy of Fallot presents with fever, poor feeding, and irritability. The nurse suspects infective endocarditis and must identify the most critical assessment finding to report immediately.
- Prioritize Life-Threatening Complications:
- Apply principles of physiological stability and risk reduction, prioritizing findings that indicate acute, irreversible organ or structural damage over non-specific or superficial signs.
- Rule in Choice 1because a change in the pitch or intensity of a baseline murmur is a direct acoustic reflection of acute structural valvular destruction or worsening cardiac obstruction.
- Eliminate Lower-Priority Options:
- Rule out Choice 2because superficial perineal skin irritation is an expected pediatric finding that carries zero risk of systemic or cardiac failure.
- Rule out Choice 3and Choice 4because mild weight loss and postprandial fatigue are general, non-specific systemic manifestations of illness rather than immediate structural cardiac emergencies.
Take home points
- A new or changing heart murmur is the most critical clinical indicator of structural cardiac destruction during infective endocarditis.
- Tetralogy of Fallot involves a ventricular septal defect, pulmonic stenosis, overriding aorta, and right ventricular hypertrophy, making its baseline hemodynamics highly sensitive to valvular infection.
- Rapid vegetation growth can cause acute valvular incompetence, leading to fulminant congestive heart failure in infants with congenital heart disease.
- Immediate reporting of acoustic cardiac changes allows for urgent echocardiographic evaluation and timely surgical or medical optimization.
The nurse is reviewing the presentation of subacute versus acute infective endocarditis in children. Which manifestations are typically characteristic of the subacute form? Select all that apply
Explanation
Subacute infective endocarditis follows an indolent, slow clinical course driven by low-virulence pathogens like Streptococcus viridans. The condition is characterized by insidious onset, constitutional symptoms resulting from persistent antigenemia, and systemic immunological deposition, causing gradual tissue degradationthat delays diagnostic confirmation.
Rationale for correct answers
1.A low-grade feverof unknown origin is the classic presentation of subacute endocarditis. The temperature elevations are frequently mild, intermittent, and can persist for weeks or months before additional localizing signs appear, masking the underlying cardiac infection.
3.The progressive anorexiaand accompanying weight loss result from chronic, low-grade systemic inflammation and metabolic consumption. Children often present with a gradual decline in energy levels, poor appetite, and general malaise that mimics a chronic systemic illness.
4.The unexplained arthralgiasand muscle aches are immunologic manifestations caused by circulating antigen-antibody complexes depositing in joint capsules and skeletal muscle microvasculature. These vague musculoskeletal complaints are common in the subacute form due to the prolonged timeline of the infection.
Rationale for incorrect answers
2.The cardiogenic shocksecondary to rapid tissue necrosis is characteristic of the fulminant, acute form of endocarditis, typically caused by Staphylococcus aureus. Subacute endocarditis allows for compensatory hemodynamic mechanisms to adapt to gradual valvular changes over months.
5.The spiking feversand rapid anatomical destruction of the valvular leaflets are hallmark features of acute infective endocarditis. Acute infection causes sudden, necrotizing structural changes within days, whereas subacute infection leads to slow, progressive fibrotic deformities.
Test-taking strategy:
- Analyze the scenario/question: The nurse is reviewing the presentation of subacute versus acute infective endocarditis in children. The question requires selecting all manifestations that are typical of the subacute form.
- Contrast Disease Timelines:
- Subacute implies a low-velocity, low-virulence process dominated by constitutional, vague, and immune-mediated signs rather than rapid structural collapse.
- Rule in Choice 1because persistent, low-grade fevers are the diagnostic hallmark of an indolent infectious process.
- Rule in Choice 3because chronic weight loss and progressive malaise reflect a slow, wasting systemic infection over weeks.
- Rule in Choice 4because a prolonged timeline allows the immune system to generate the complexes responsible for joint and muscle pains.
- Eliminate Acute Indicators:
- Rule out Choice 2and Choice 5because rapid hemodynamic collapse, shock, high fevers, and acute perforation are dangerous, high-velocity features exclusive to acute pyogenic infections.
Take home points
- Subacute infective endocarditis is characterized by an insidious onset with vague, non-specific symptoms that can persist for months.
- Low-virulence oral commensals such as Viridans group streptococci are the primary causative agents of subacute endocardial infections.
- Prolonged systemic bacteremia in subacute disease leads to circulating immune complex deposition, causing arthralgias and splenomegaly.
- Acute endocarditis presents with high fevers and rapid valvular destruction, demanding immediate empiric antimicrobial therapy.
The nurse notes thin, linear, dark-red streaks under the nail beds of a child admitted for structural heart disease and prolonged fever. The nurse documents these as:
Explanation
Peripheral cutaneous and subungual manifestations provide critical diagnostic clues for infective endocarditis, reflecting distinct underlying pathophysiological processes. Linear micro-bleed patterns beneath the nails arise from microembolic vascular phenomenaor localized capillary damage, whereas discrete skin lesions represent immunological depositionor direct septic microinfarction, requiring precise clinical differentiation to track systemic complications.
Rationale for correct answer
3.The splinter hemorrhagespresent as thin, linear, dark-red streaks running longitudinally beneath the nail beds. They are caused by septic microemboli dislodged from cardiac vegetations that damage the subungual capillaries, leading to localized extravasation of red blood cells along the epidermal ridges.
Rationale for incorrect answers
1.The Osler nodesare painful, tender, raised nodules that characteristically develop on the pads of the fingers and toes. Unlike splinter hemorrhages, they are immunologic phenomena caused by the deposition of circulating immune complexes in the local cutaneous vasculature rather than linear vascular streaks under the nail.
2.The Janeway lesionsare non-tender, flat, erythematous macules that typically appear on the palms of the hands and soles of the feet. They represent vascular phenomena caused by septic microembolization, but they are morphologically and anatomically distinct from longitudinal subungual capillary streaks.
4.The petechiaepresent as tiny, circular, non-blanching red or purple spots caused by minor intradermal capillary bleeding. While petechiae frequently occur in infective endocarditis across the conjunctivae, oral mucosa, and skin, they do not present as thin, linear streaks restricted to the subungual tissue.
Test-taking strategy:
- Analyze the scenario/question: The nurse observes thin, linear, dark-red streaks under the nail beds of a child with structural heart disease and prolonged fever. The nurse must identify the correct clinical term for this finding.
- Identify Anatomical Locations:
- Restrict choices based on the specific anatomical zone described; the question details a linear vascular manifestation located exclusively under the fingernails or toenails.
- Rule in Choice 3because splinter hemorrhages match the description of being longitudinal, dark-red capillary streaks situated beneath the nail plate.
- Eliminate Incompatible Alternatives:
- Rule out Choice 1because Osler nodes are painful, raised nodules located on the fleshy skin pads of the distal digits.
- Rule out Choice 2because Janeway lesions are flat, painless macules scattered across the broad skin surfaces of the palms and soles.
- Rule out Choice 4because petechiae are small, pinpoint, circular hemorrhagic spots rather than elongated linear subungual lines.
Take home points
- Splinter hemorrhages are thin, linear, longitudinal dark-red lines appearing under the nail beds caused by microembolic capillary damage.
- Osler nodes are painful, raised nodules on the distal finger and toe pads driven by localized immune complex deposition.
- Janeway lesions are painless, erythematous macules on the palms and soles caused by septic microemboli from cardiac vegetations.
- Peripheral vascular and immunologic signs are categorized as minor criteria under the Modified Duke Criteria for diagnosing infective endocarditis.
The nurse is caring for a child with native valve endocarditis (NVE). The nurse understands that this classification means the infection:
Explanation
Infective endocarditis is classified anatomically based on the nature of the target tissue surface. Native valve endocarditis refers to an active microbial infection involving the endocardial surfaceof the patient's own autologous heart valves, whether those valves are structurally normal or possess congenital anomalies, differentiating it from infections that colonize bioprosthetic implants.
Rationale for correct answer
2.The native valveclassification specifies that the target site of infection is the child's natural cardiac structure. This includes structurally normal valves or valves deformed by congenital conditions, provided no prosthetic or synthetic material has replaced the natural tissue substrate.
Rationale for incorrect answers
1.An infection on a surgically replaced mechanical device is classified as prosthetic valve endocarditisrather than native valve endocarditis. This distinction is critical because prosthetic infections involve foreign material, carry a higher mortality rate, and often require completely different surgical and pharmacological treatments.
3.An infection strictly limited to the lining of the inferior vena cava does not constitute native valve endocarditis. While intravascular infections can occur, endocarditis is pathologically defined by the infection of the endocardial liningof the heart chambers and its associated valvular structures.
4.The neonatal unitorigin describes a nosocomial or healthcare-associated acquisition pathway rather than an anatomical classification. Native valve endocarditis can be acquired in any setting, including community or nosocomial environments, as the term refers solely to the anatomical structure infected.
Test-taking strategy:
- Analyze the scenario/question: The nurse is caring for a child with native valve endocarditis. The question requires defining what this specific medical classification means regarding the site of infection.
- Decode Medical Terminology:
- The word "native" in a clinical context refers to the patient's own biological tissue or organs, as opposed to artificial, prosthetic, or transplanted components.
- Rule in Choice 2because it accurately defines native valve endocarditis as an infection occurring on the patient's own natural or congenitally altered cardiac valves.
- Eliminate Incompatible Classes:
- Rule out Choice 1because infections on mechanical or bioprosthetic materials are categorized under prosthetic valve endocarditis.
- Rule out Choice 3because the inferior vena cava is an extra-cardiac great vessel, not a cardiac valve.
- Rule out Choice 4because epidemiological origins (nosocomial versus community-acquired) are distinct from anatomical tissue classifications.
Take home points
- Native valve endocarditis describes an infection localized to the patient's own natural heart valves.
- The classification stands in direct contrast to prosthetic valve endocarditis, which involves synthetic or transplanted tissue.
- Native valves may be structurally healthy or may possess pre-existing anomalies like bicuspid aortic valves or rheumatic scars.
- Differentiating between native and prosthetic valve infection dictates the choice, duration, and surgical threshold of antibiotic therapy.
Exams on Acquired Cardiovascular Disorders: Infective Endocarditis
Custom Exams
Login to Create a Quiz
Click here to loginLessons
- Practice Excercise 3
- Summary
- Comprehensive Questions
- Objectives
- Introduction
- Epidemiology, Etiology, Risk Factors, And Pathophysiology
- Practice Excercise 1
- Clinical Manifestations
- Classification
- Diagnostic Evaluation
- Practice Excercise 2
- Therapeutic Management
- Nursing Care Plan
- Complications
- Prognosis
- Prevention
Notes Highlighting is available once you sign in. Login Here.
Summary
- Infective endocarditis (IE) represents a high-stakes, life-threatening cardiovascular infection in pediatric nursing practice.
- Although once predominantly tied to the systemic consequences of untreated rheumatic fever, the contemporary landscape of pediatric IE is primarily dominated by two populations: children surviving with complex, surgically altered congenital heart disease (CHD), and vulnerable pediatric patients requiring long-term central venous lines.
- The core pathology involves high-velocity turbulent blood flow that damages endocardial surfaces, triggering a localized fibrin-platelet matrix that acts as a landing strip for circulating bacteria or fungi.
- Once colonized, these pathogens construct a protective, avascular vegetation biofilm that isolates them from standard immune defenses and limits antibiotic penetration.
- Diagnosing pediatric IE requires synthesizing clinical parameters using the Modified Duke Criteria.
- Nurses must remain vigilant for vague, prolonged constitutional cues like low-grade fevers, progressive fatigue, and failure to thrive in infants, alongside cardiac markers like a new or changing regurgitant murmur.
- Securing accurate diagnostic data demands that the nurse draw at least three independent sets of blood cultures from separate peripheral sites before the initiation of any antimicrobial agents.
- Management centers on a rigorous, 4-to-6-week regimen of high-dose, bactericidal intravenous antibiotics, alongside close monitoring for severe complications such as acute congestive heart failure, conduction blocks, and systemic embolic events like strokes or pulmonary infarctions.
- For high-risk cohorts, preventative care remains paramount. Nurses must champion strict compliance with American Heart Association guidelines, ensuring that families understand the mandate for prophylactic Amoxicillin administration (50 mg/kg) prior to invasive dental procedures.
- Through prompt clinical identification, meticulously executed central line maintenance, and proactive family education, pediatric nurses directly reduce the mortality and long-term valvular morbidity associated with this complex cardiovascular disorder.
Objectives
- Differentiate between the distinct clinical manifestations of acute versus subacute infective endocarditis (IE) in the pediatric population.
- Analyze the predisposing risk factors for pediatric IE, specifically evaluating the roles of underlying congenital heart disease (CHD), prosthetic materials, and indwelling central venous catheters.
- Explain the step-by-step pathophysiology of non-bacterial thrombotic endocarditis (NBTE) shifting into active microcolony vegetation.
- Apply the Modified Duke Criteria (incorporating the 2023 updates) to establish a clinical diagnosis of definite or possible IE based on laboratory, microbiological, and imaging findings.
- Formulate comprehensive nursing care plans focusing on long-term intravenous antimicrobial administration, central line maintenance, and hemodynamic monitoring.
- Identify critical systemic complications of IE, including septic embolization, valvular insufficiency, and acute heart failure.
- Synthesize evidence-based patient and family teaching guidelines regarding mandatory antibiotic prophylaxis for high-risk pediatric populations prior to invasive procedures.
Introduction
- Infective endocarditis (IE) is a rare but potentially catastrophic microbial infection affecting the endocardial surface of the heart, its valves, or surgically implanted prosthetic materials and conduits.
- Although historically linked to rheumatic heart disease (RHD), the contemporary epidemiology of pediatric IE has shifted significantly in developed countries.
- Today, it presents primarily as an acquired complication in children with underlying structural congenital heart defects (CHD) or as an iatrogenic infection resulting from prolonged use of indwelling central venous lines in critically ill neonates and pediatric oncology patients.
- The pathogenesis of this condition centers on endocardial endothelial damage caused by high-velocity or turbulent blood flow. This trauma triggers a localized clotting cascade, forming a microscopic matrix of fibrin and platelets.
- When bacteremia or fungemia occurs, frequently via routine activities like vigorous tooth brushing or through invasive medical procedures, pathogens colonize this matrix, sealing themselves beneath layers of clotting factors to create a protective biofilm or "vegetation."
- From a nursing perspective, recognizing pediatric IE requires a high index of suspicion because its early clinical cues are notoriously subtle, vague, and variable.
- Unlike adults, children often lack classical peripheral immunologic or vascular phenomena. Instead, they present with persistent, unexplained low-grade fevers, progressive fatigue, and feeding intolerance that can easily mimic routine childhood viral illnesses.
- Nurses play a pivotal role in the early detection, management, and prevention of this life-threatening disorder.
- Care requires executing a rigorous, weeks-long regimen of intravenous antimicrobial therapy, protecting central vascular access devices, monitoring for acute heart failure or embolic strokes, and delivering essential family education regarding prophylactic antibiotic protocols.
- Early intervention remains paramount to preventing irreversible valvular destruction, cardiogenic shock, or severe neurologic impairment.
Epidemiology, Etiology, Risk Factors, And Pathophysiology
Epidemiology
Pediatric infective endocarditis is a low-incidence but high-morbidity disorder. It accounts for approximately 0.05 to 0.78 cases per 1,000 pediatric hospital admissions annually. While the disease is rare, its incidence has trended upward over the last few decades. This rise is paradoxically tied to medical advancements: a greater population of children with complex congenital heart diseases now survive long-term due to complex surgical corrections, creating a larger permanent pool of at-risk hosts. Mortality rates remain significant, hovering between 5% and 15% depending on the causative pathogen and the child's underlying anatomy.
Etiology
Gram-positive bacteria remain the dominant causative agents in pediatric IE, accounting for more than 80% of documented cases:
- Viridans Group Streptococci (e.g., S. mitis, S. mutans): Historically the most common cause in children with underlying structural heart defects following dental procedures or oral trauma. They tend to follow a subacute, more gradual clinical course.
- Staphylococcus aureus: The leading cause of acute infective endocarditis. It is highly aggressive and capable of invading entirely normal, structurally sound heart valves. It is increasingly prevalent due to hospital-acquired infections, surgical site contamination, and intravenous drug use in adolescents. Methicillin-Resistant S. aureus (MRSA) significantly complicates treatment.
- Coagulase-Negative Staphylococci (e.g., Staphylococcus epidermidis): Heavily associated with prosthetic heart valves, patches, patches or conduits, and long-standing central venous lines.
- HACEK Group: (Haemophilus, Aggregatibacter, Cardiobacterium, Eikenella, Kingella). A group of fastidious, slow-growing Gram-negative organisms that are difficult to culture but represent a notable subset of community-acquired pediatric cases.
- Fungal Organisms (e.g., Candida albicans, Aspergillus): Highly lethal variant primarily seen in profoundly immunosuppressed children, low-birth-weight neonates in the NICU, or those following open-heart surgery with prolonged broad-spectrum antibiotic exposure.
Risk Factors
Pediatric patients can be stratified by risk based on anatomical and environmental factors:
|
Risk Category |
Clinical Manifestations & Structural Examples |
|
Highest Risk |
• Prosthetic heart valves (mechanical or bioprosthetic). • Previous history of infective endocarditis. • Unrepaired cyanotic congenital heart defects (e.g., Tetralogy of Fallot, Transposition of the Great Arteries). • Surgically constructed systemic-to-pulmonary shunts or conduits (e.g., Blalock-Taussig shunt). • Surgical repairs using prosthetic material or devices within the first 6 months post-procedure. |
|
Moderate Risk |
• Unrepaired acyanotic structural defects (e.g., Ventricular Septal Defect [VSD], Coarctation of the Aorta). • Hypertrophic cardiomyopathy. • Acquired valvular dysfunction (e.g., Rheumatic heart disease causing permanent scarring and leaflet thickening). |
|
Low/No Risk |
• Small, isolated, unrepaired Atrial Septal Defects (ASD) (low pressure gradients generate minimal turbulence). • History of innocent, musical heart murmurs with normal structural anatomy. • Surgical closure of an ASD or VSD past 6 months without residual defects. |
|
Environmental/Healthcare Risk |
• Indwelling central venous access devices (e.g., Central lines, PICC lines) causing mechanical endothelial trauma. • Intravenous drug use (IVDU) in adolescent populations, introducing pathogens directly into the systemic venous circulation. |
Pathophysiology
The mechanical evolution of infective endocarditis follows a distinct sequence of endothelial trauma and microbial colonization:
- Endocardial Damage: High-velocity regurgitant jets or turbulent blood flow across anatomical narrowing (e.g., a VSD or stenotic valve) strips or alters the normal endothelial lining of the heart.
- Non-Bacterial Thrombotic Endocarditis (NBTE): In response to the endothelial injury, the body's natural hemostatic repair mechanisms deposit a localized matrix of fibrin and platelets onto the denuded surface, forming a sterile clot.
- Transient Bacteremia: Microorganisms enter the bloodstream via everyday micro-trauma (e.g., dental cleanings, aggressive flossing, skin infections) or medical manipulations (e.g., accessing a central line).
- Adherence and Colonization: Circulating bacteria adhere to the sticky fibrin-platelet matrix of the NBTE. Certain pathogens, like S. aureus, produce surface adhesins that bind aggressively to fibronectin.
- Vegetation Maturation: Once attached, the bacteria multiply rapidly and stimulate further platelet aggregation and fibrin deposition over themselves. This creates an expanding mass called a vegetation. The layering of fibrin shields the bacteria from host white blood cells and limits antibiotic penetration, creating a highly protective, avascular biofilm microenvironment.
- Local and Systemic Destruction: The expanding vegetation causes direct, irreversible destruction of underlying valvular leaflets, chordae tendineae, or septal structures. Concurrently, fragments of the brittle vegetation break off into the high-pressure arterial circulation, causing septic downstream embolization.
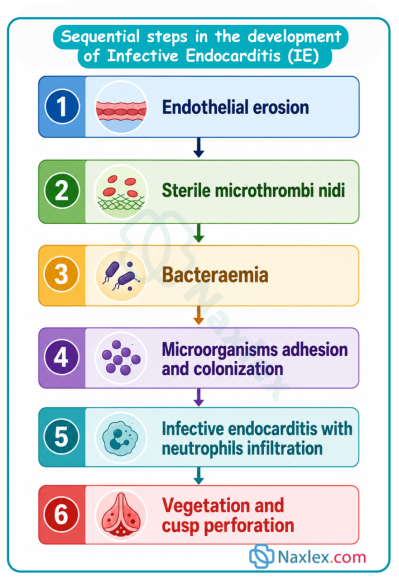
Clinical Manifestations
The clinical signs of pediatric IE vary widely depending on whether the infection is acute (rapidly progressive, high fevers, toxic appearance) or subacute (indolent, prolonged low-grade fevers, progressive weight loss).
Classic Constitutional Signs
- Fever: Present in over 85% to 90% of pediatric patients. In subacute cases, it can be intermittent and low-grade, often unaccompanied by obvious localizing symptoms.
- Malaise, Lethargy, and Anorexia: Infants present with marked feeding intolerance, falling asleep during bottle feeds and showing a distinct pattern of failure to thrive (FTT).
- Tachycardia and Tachypnea: Out of proportion to the degree of fever, reflecting early compensatory mechanisms for cardiovascular stress.
Cardiac-Specific Signs
- New or Changing Heart Murmur: Found in standard clinical exams. A shifting or completely new regurgitant murmur indicates active valvular structural destruction (e.g., worsening mitral or aortic insufficiency).
- Congestive Heart Failure (CHF) Manifestations: Dyspnea, periorbital edema, hepatomegaly, gallop rhythms (S3), and increased work of breathing as a consequence of acute valvular incompetence.
Extracardiac/Peripheral Phenomena (Less common in young children than in adults)
- Vascular Phenomena (Embolic):
- Petechiae: Tiny, pinpoint non-blanching hemorrhages located on the palpebral conjunctiva, buccal mucosa, or extremities.
- Splinter Hemorrhages: Linear, dark-red streaks running longitudinally underneath the nail beds.
- Janeway Lesions: Flat, painless, erythematous or hemorrhagic macules located on the palms of the hands and soles of the feet. These represent septic microemboli.
- Immunologic Phenomena (Immune-Complex Mediated):
- Osler Nodes: Tender, painful, raised pea-sized pea-sized nodules typically found on the pads of the fingers and toes.
- Roth Spots: Oval, retinal hemorrhages with pale, white centers seen during an ophthalmoscopic exam.
- Glomerulonephritis: Manifesting clinically as microscopic hematuria (>50% of cases) and proteinuria due to immune complexes trapping in the renal basement membrane.
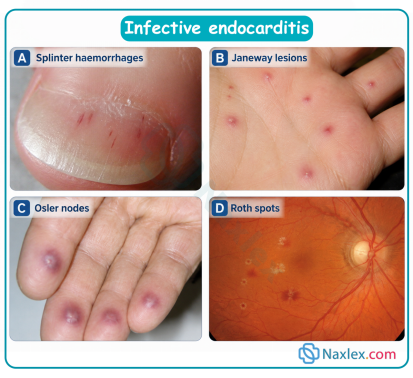
Classification
Classification by Valve Type and Substrate
- Native Valve Endocarditis (NVE): Infection occurring on the child’s natural structural valves. It is split between those with pre-existing defects (CHD) and those with structurally normal hearts (frequently S. aureus in older children or adolescents).
- Prosthetic Valve Endocarditis (PVE): Occurs on mechanical or bioprosthetic valves, synthetic patches (e.g., Dacron or Gore-Tex patches used for VSD closure), or artificial conduits. PVE is sub-classified into:
- Early PVE: Occurring within 12 months of cardiac surgery (often tracking back to intraoperative or immediate post-operative nosocomial contamination).
- Late PVE: Occurring more than 12 months post-operatively (resembling community-acquired infections).
Classification by Clinical Course and Duration
- Acute Infective Endocarditis: Characterized by rapid, fulminant onset over days, marked by high septic fevers, severe constitutional toxicity, rapid valvular perforation, and a high propensity for early septic embolization. Typically driven by Staphylococcus aureus.
- Subacute Infective Endocarditis: Evolves insidiously over weeks to months, with subtle, low-grade fevers, night sweats, unexplained weight loss, and vague musculoskeletal joint aches. Most commonly driven by Viridans Group Streptococci.
Classification by Location / Chamber Lateralization
- Left-Sided Endocarditis: Involves the mitral or aortic valves. This form presents a high risk for systemic arterial embolization to the brain (stroke), spleen, kidneys, and extremities.
- Right-Sided Endocarditis: Involves the tricuspid or pulmonary valves. This is highly common in children with indwelling central lines or specific congenital lesions like Tetralogy of Fallot or VSDs (where the jet shoots rightward). Fragments break off into the pulmonary circulation, causing septic pulmonary embolisms, localized infarctions, and pneumonia-like infiltrates.
Diagnostic Evaluation
The definitive clinical diagnosis of pediatric infective endocarditis relies heavily on the Modified Duke Criteria. Diagnosis requires a synthesis of microbiological data, advanced cardiac imaging, and clinical assessments.
Laboratory Evaluation
- Blood Cultures (The Diagnostic Gold Standard):
Critical Nursing Action: Obtain at least three independent sets of blood cultures drawn from separate venipuncture sites prior to administering the first dose of empiric antibiotic therapy. Each draw must include adequate volume based on pediatric weight guidelines.
For stable, subacute cases, spacing draws out over 24 hours can catch intermittent bacteremia. For critically ill or unstable patients with suspected acute IE, all three sets can be drawn within 1 to 2 hours from distinct anatomical sites to prevent delaying targeted therapy.
- Inflammatory Markers: Erythrocyte Sedimentation Rate (ESR) and C-Reactive Protein (CRP) are almost universally elevated but are non-specific indicators of active systemic inflammation.
- Complete Blood Count (CBC): Reveals a normocytic, normochromic anemia of chronic disease alongside a marked leukocytosis with a left shift in acute presentations.
- Urinalysis: Routinely checked for microscopic hematuria or proteinuria, which serves as a key indicator of immunologic renal involvement (glomerulonephritis) or embolic renal infarction.
Imaging Evaluation
- Transthoracic Echocardiogram (TTE): The primary, non-invasive initial test utilized in children. It allows visual identification of oscillating intracardiac masses (vegetations), structural abscesses, new or worsening valvular regurgitation, or partial dehiscence of a prosthetic patch or valve.
- Transesophageal Echocardiogram (TEE): Indicated if TTE views are technically limited by a patient's body habitus, chest walls, or if there is extensive prosthetic hardware obscuring the view. It provides exceptional resolution of the posterior structures, including mechanical mitral and aortic valves.
Application of the Modified Duke Criteria
To declare a diagnosis of Definite IE, a patient must meet specific combinations of major and minor criteria:
Major Criteria
- Positive Blood Cultures: Typical microorganisms identified from two separate blood cultures (S. viridans, S. aureus, HACEK group) or persistently positive blood cultures drawn more than 12 hours apart.
- Evidence of Endocardial Involvement: Positive echocardiogram demonstrating an oscillating intracardiac mass (vegetation) on a valve or supporting structure, a myocardial abscess, or new partial dehiscence of a prosthetic valve; OR a new valvular regurgitation/murmur.
Minor Criteria
- Predisposition: High-risk cardiac condition (predisposing CHD, prosthetic valve) or a history of IV drug use.
- Fever: Documented temperature greater than 38°C (100.4°F).
- Vascular Phenomena: Major arterial emboli, septic pulmonary infarcts, mycotic aneurysms, intracranial hemorrhages, Janeway lesions, or conjunctival hemorrhages.
- Immunological Phenomena: Glomerulonephritis, Osler nodes, Roth spots, or a positive rheumatoid factor.
- Microbiological Evidence: Positive blood cultures that do not meet a major criterion, or serological evidence of active infection with an organism consistent with IE.
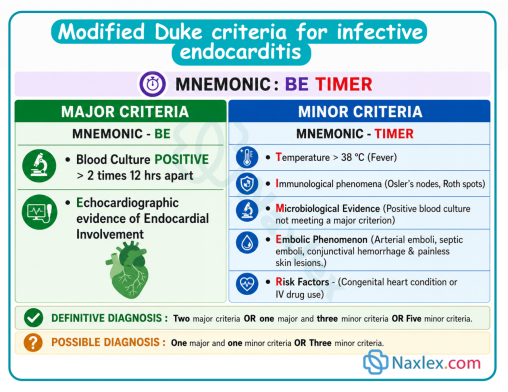
Therapeutic Management
Medical Management
The management of pediatric IE relies on high-dose, bactericidal intravenous antibiotic therapy delivered over an extended duration, typically lasting 4 to 6 weeks. Because the bacterial colony inside a vegetation is embedded within a dense, avascular biofilm of fibrin, standard oral doses or short courses are completely ineffective.
- Empiric Therapy: Initiated immediately after blood cultures are drawn for clinically unstable patients. The choice is tailored toward covering the most probable organisms:
- Native Valve Suspected IE: Often a combination of Ampicillin (or Penicillin G) combined with Gentamicin to leverage a synergistic bactericidal effect. Alternatively, Ceftriaxone may be utilized.
- Prosthetic Valve or Healthcare-Associated Suspected IE: Typically requires broad-spectrum coverage with Vancomycin (to cover MRSA and resistant staphylococci) paired with Gentamicin or Rifampin (which penetrates biofilms on synthetic hardware effectively).
- Targeted Therapy: Once the specific pathogen is isolated and its minimum inhibitory concentration (MIC) sensitivities are finalized, the medical team de-escalates or alters the drug regimen to the narrowest, most effective agent.
- Serum Drug Monitoring: Essential for medications with narrow therapeutic windows. Nurses must coordinate timely draws for Vancomycin troughs and Gentamicin peaks/troughs to maximize therapeutic killing while minimizing the risks of permanent nephrotoxicity or ototoxicity.
Surgical Management
Approximately 20% to 30% of pediatric patients require emergency or urgent operative intervention (open-heart surgery) before their 6-week antibiotic course is finished. Indications for surgical intervention include:
- Refractory Congestive Heart Failure (CHF): Severe, worsening cardiac failure secondary to acute valvular disruption or structural regular leak that fails to respond to aggressive diuretic therapy.
- Uncontrolled Infection: Persistent bacteremia or high spiking fevers despite more than 7 to 10 days of targeted, appropriate antimicrobial therapy, indicating abscess formation or a drug-resistant biofilm.
- High Embolic Risk: Echocardiographic visualization of exceptionally large (>10 mm to 15 mm in size), highly mobile vegetations, especially when coupled with episodes of recurrent systemic embolization.
- Fungal Endocarditis: Antifungal drugs are rarely capable of sterilizing fungal vegetations; standard care dictates early, radical surgical debridement and valve reconstruction.
Nursing Care Plan
Pediatric nursing care for infective endocarditis centers on prolonged intravenous therapy management, minimizing cardiac workload, monitoring for systemic embolic events, and tracking drug-related toxicities.
Nursing Diagnosis 1: Decreased Cardiac Output
- Related to: Altered valvular structure and function (regurgitation or stenosis) secondary to microbial tissue destruction.
- Evidenced by: Tachycardia, tachypnea, developmental feeding exhaustion, diminished peripheral pulses, gallop rhythms, and active periorbital edema.
- Nursing Interventions:
- Assess and document core vital signs every 2 to 4 hours, carefully observing for sudden drops in blood pressure or increases in resting heart rate.
- Auscultate cardiac sounds for the development of any new murmurs or changes in the acoustic character of an existing murmur.
- Administer prescribed cardiac medications (e.g., loop diuretics like Furosemide, afterload reducers like ACE inhibitors) as ordered, and strictly track hourly intake and output (I/O).
- Cluster nursing cares to provide periods of uninterrupted rest, minimizing the child's metabolic and cardiac oxygen demands.
- Expected Outcomes: The child exhibits stable hemodynamics, clear breath sounds, adequate urine output (>1 mL/kg/hour for infants, >0.5 mL/kg/hour for older children), and a return to baseline respiratory effort.
Nursing Diagnosis 2: Risk for Injury / Altered Tissue Perfusion (Systemic/Pulmonary)
- Related to: Fragmentation and dislodgement of brittle intracardiac vegetations into the systemic or pulmonary arterial circulations.
- Evidenced by: Potential for focal neurological deficits, acute abdominal pain, or sudden chest pain with respiratory distress.
- Nursing Interventions:
- Perform comprehensive neurological assessments (pupillary responses, level of consciousness, symmetric motor movement of all four extremities) every 4 to 8 hours.
- Monitor for sudden-onset complications based on the anatomical location of the vegetation:
- Left-sided vegetations: Assess for signs of embolic stroke (facial drooping, asymmetric weakness), acute renal infarction (sudden flank pain, gross hematuria), or splenic infarction (acute left upper quadrant abdominal pain).
- Right-sided vegetations: Monitor for sudden dyspnea, localized pleuritic chest pain, coughing up blood (hemoptysis), or an abrupt drop in oxygen saturation (SpO2), signaling a septic pulmonary embolism.
- Maintain the patient on appropriate activity restrictions during the initial phase of therapy when vegetations are highly mobile.
- Expected Outcomes: The patient maintains intact perfusion across all major organ systems with zero signs of focal neurological deficits or acute respiratory decompensation.
Nursing Diagnosis 3: Risk for Infection / Deficient Central Line Maintenance
- Related to: The mandatory presence of long-term central venous access devices (PICC lines or tunneled catheters) required for a 6-week course of highly irritating antibiotics.
- Evidenced by: Erythema, swelling, or purulent drainage at the insertion site, or new central line-associated blood stream infections (CLABSIs).
- Nursing Interventions:
- Inspect the central venous access insertion site hourly during continuous infusions for signs of redness, tracking, swelling, or dressing lift.
- Perform all central line dressing changes, line accesses, and cap changes utilizing strict aseptic technique according to institutional CLABSI prevention bundles.
- Ensure correct flushing protocols using appropriate volumes of saline and heparin to maintain line patency and avoid intraluminal clot formation.
- Monitor the patient's daily temperature curve; investigate any sudden spike in temperature occurring shortly after a central line is flushed.
- Expected Outcomes: The central line site remains clean, dry, and intact, and the patient successfully completes the 6-week antibiotic regimen without developing an iatrogenic line infection.
Complications
- Acute Congestive Heart Failure: The single most common complication of pediatric IE. It occurs when a valve leaflet is perforated or a chordae tendineae ruptures, creating an abrupt volume overload that the myocardium cannot accommodate.
- Septic Embolization and Infarctions:
- Central Nervous System: Septic cerebral emboli can cause ischemic strokes, intracerebral abscesses, or toxic mycotic aneurysms (weakened, infected arterial walls that carry a high risk for catastrophic rupture and hemorrhagic stroke).
- Pulmonary System: Right-sided fragments lead to multiple cavities, lung abscesses, and septic infarctions.
- Myocardial Abscess and Conduction Blocks: The infection can track downward from the valve annulus into the adjacent cardiac conduction pathways (such as the AV node or Bundle of His). This can manifest on an ECG as a new, progressive first-degree heart block or higher-degree AV blocks.
- Immune-Complex Glomerulonephritis: Chronic antigen-antibody complexes settle within the renal filters, potentially leading to acute kidney injury (AKI) or chronic renal insufficiency.
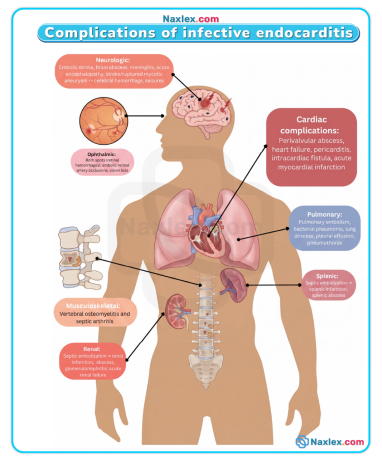
Prognosis
The ultimate prognosis for a child diagnosed with infective endocarditis depends heavily on three key variables: the virulence of the isolated microorganism, the presence of pre-existing complex CHD, and the speed at which appropriate bactericidal therapy was initiated.
- Streptococcal Endocarditis: When caused by penicillin-sensitive Viridans Group Streptococci, the cure rate exceeds 90% to 95% with low long-term morbidity.
- Staphylococcal and Fungal Endocarditis: S. aureus infections carry a much more guarded prognosis, with mortality rates scaling up to 20% due to rapid tissue destruction and early neurological embolic events. Fungal IE carries an exceptionally high mortality rate, often exceeding 50%.
- Long-Term Sequelae: Surviving children require lifelong longitudinal follow-up with a pediatric cardiologist. A substantial portion will require future elective operations later in life to reconstruct or replace damaged, scarred valves that became progressively regurgitant over time.
Prevention
For high-risk pediatric populations, prevention is the cornerstone of clinical management. The American Heart Association (AHA) and American Academy of Pediatric Dentistry establish clear guidelines regarding who must receive antibiotic prophylaxis prior to specific invasive procedures.
Who Requires Prophylaxis? (High-Risk Groups Only)
- Prosthetic Heart Valves: Any child with a mechanical or bioprosthetic valve or those who have had a prosthetic material utilized for a cardiac valve repair.
- Previous History of IE: Any child who has survived a prior episode of infective endocarditis, regardless of whether they have structural heart disease.
- Unrepaired Cyanotic Congenital Heart Disease: Including palliative shunts and conduits.
- Completely Repaired CHD with Prosthetic Material: Only during the first 6 months following the surgical or transcatheter procedure (allowing time for the endothelial tissue to fully grow over and protect the synthetic material).
- Repaired CHD with Residual Defects: Any repaired defect that retains a residual leak or shunt at or adjacent to the site of a prosthetic patch or device (which perpetually generates localized turbulence).
- Cardiac Transplant Recipients: Those who develop subsequent cardiac valvulopathy.
Which Procedures Require Prophylaxis?
- Dental Procedures: Any manipulation involving the gingival tissues, the periapical region of teeth, or perforation of the oral mucosa (e.g., routine dental cleanings, extractions, biopsy, scaling).
- Invasive Respiratory Procedures: Only those involving an incision or biopsy of the respiratory mucosa (e.g., a rigid bronchoscopy with biopsy, tonsillectomy, or adenoidectomy).
- Nursing insight: Routine GI or GU procedures (such as standard upper endoscopies or urinary catheterizations) no longer routinely require IE prophylaxis unless an active infection is being treated.
Standard Pharmacological Prophylactic Regimen
- First-Line Agent: Amoxicillin administered as a single oral dose given 30 to 60 minutes prior to the scheduled procedure.
- Pediatric Dosage: 50 mg/kg (maximum absolute dose of 2 grams).
- Alternative for Penicillin-Allergic Patients: Cephalexin (50 mg/kg), Clindamycin (20 mg/kg), or Azithromycin/Clarithromycin (15 mg/kg).
Naxlex
Videos
Login to View Video
Click here to loginTake Notes on Acquired Cardiovascular Disorders: Infective Endocarditis
This filled cannot be empty
Join Naxlex Nursing for nursing questions & guides! Sign Up Now
