
Please set your exam date
Binge-Eating Disorder
Study Questions
Practice Questions 1
The nurse is assessing a client suspected of having binge-eating disorder. Which of the following findings best distinguishes this disorder from bulimia nervosa?
Explanation
Binge-eating disorder entails recurrent episodes of excessive food consumption without regular compensatory behaviors. Unlike bulimia nervosa, which involves purging or excessive exercise to prevent weight gain, this condition often results in significant obesity and associated metabolic comorbidities.
Rationale for correct answers:
C. Binge-eating disorder is distinguished from bulimia nervosa by the absence of recurrent compensatory behaviors. Patients with bulimia nervosa systematically employ methods to negate caloric intake, whereas this specific diagnostic criterion differentiates the binge-eating clinical presentation.
Rationale for incorrect answers:
A. The consumption of an objectively large amount of food within a discrete period is a core diagnostic feature common to both binge-eating and bulimia nervosa. This observation alone does not provide the clinical distinction necessary to differentiate between these two distinct psychiatric eating disorders.
B. A subjective sense of loss of control during an eating episode is a mandatory diagnostic criterion for both binge-eating and bulimia nervosa. This shared psychological experience fails to serve as a distinguishing factor between the two clinical diagnoses during an assessment.
D. Experiencing marked distress and guilt following eating episodes is a characteristic psychological response observed in both binge-eating and bulimia nervosa. This emotional state is common to both conditions and does not offer diagnostic utility for distinguishing one from the other.
Test-taking strategy:
Analyze the scenario/question: The question asks to identify the specific diagnostic criterion that differentiates binge-eating disorder from bulimia nervosa.
Apply knowledge of diagnostic criteria: To answer this question, analyze the pathophysiology and behavioral diagnostic criteria for both eating disorders. Both disorders involve episodic overeating and subsequent psychological distress.
- Rule out Choice 1: Both disorders define binge episodes by the consumption of objectively large amounts of food in a short timeframe.
- Rule out Choice 2: The feeling of a loss of control is a core diagnostic requirement present in both clinical manifestations.
- Rule in Choice 3: This is the defining feature; bulimia nervosa requires compensatory mechanisms, while binge-eating disorder does not.
- Rule out Choice 4: Significant guilt and distress are universal findings following binge episodes in both patient populations.
Take home points
- Binge-eating disorder is characterized by recurrent episodes of overeating without inappropriate compensatory behaviors
- Bulimia nervosa requires the presence of recurrent compensatory behaviors such as purging or excessive exercise
- Loss of control and post-binge distress are shared features of both eating disorders
- Differentiation relies on the absence or presence of compensatory mechanisms to prevent weight gain
The nurse is teaching a community group about the epidemiology of eating disorders. Which of the following statements about binge-eating disorder is accurate for the nurse to include?
Explanation
Binge-eating disorder represents a prevalent psychiatric condition characterized by recurring episodes of overeating. It impacts diverse demographic groups across the lifespan, frequently leading to significant metabolic health challenges and psychological morbidity.
Rationale for correct answers:
B. Epidemiological data confirms that binge-eating disorder is the most common eating disorder in the general population. Research indicates a higher lifetime prevalence compared to both anorexia nervosa and bulimia nervosa among various age and gender groups.
Rationale for incorrect answers:
A. This disorder does not occur exclusively in affluent adolescents but affects individuals across all socioeconomic levels. It is prevalent in adults of all ages and diverse cultural backgrounds rather than being limited to one group.
C. Prevalence studies demonstrate a more balanced gender distribution than other eating disorders, with a ratio closer to 1.5:1. It significantly affects both males and females across the general population without such extreme disparity.
D. Diagnostic criteria do not require a body mass index exceeding 30 kg/m² for a diagnosis. While often comorbid with obesity, the disorder is diagnosed based on behavioral patterns regardless of the specific weight or adiposity status.
Test-taking strategy:
Analyze the scenario/question: The nurse is educating a community group about the epidemiology of binge-eating disorder. The goal is to identify the statement that accurately reflects current clinical prevalence and diagnostic criteria.
Apply knowledge of epidemiological trends: Evaluate each statement based on established psychiatric statistics regarding eating disorders. Compare known prevalence data for binge-eating disorder against other eating pathologies.
- Rule out Choice 1: Binge-eating disorder is not restricted to affluent adolescent females; it occurs across the lifespan and across diverse socioeconomic statuses.
- Rule in Choice 2: Epidemiological evidence consistently identifies binge-eating disorder as having the highest prevalence rate among all recognized eating disorders in the general population.
- Rule out Choice 3: The gender ratio is not 10:1, which is more characteristic of other specific eating disorders; the actual distribution is far more equitable between genders.
- Rule out Choice 4: Obesity is a frequent correlate but not a diagnostic necessity; a client can meet criteria for binge-eating disorder at various weight categories.
Take home points
- Binge-eating disorder is the most prevalent eating disorder among the general population
- The condition affects both males and females with a relatively similar frequency
- Clinical diagnosis depends on behavioral symptoms rather than a specific body mass index threshold
- Socioeconomic status does not serve as a limiting factor for the development of the disorder
The nurse is identifying factors that increase a client's vulnerability to binge-eating disorder. Which of the following are recognized risk factors? Select all that apply
Explanation
Binge-eating disorder etiology involves multifactorial developmental pathways influenced by early childhood experiences and biological predispositions. Understanding these vulnerabilities allows for targeted clinical interventions and early identification of individuals at high risk for developing disordered eating patterns.
Rationale for correct answers:
A. Childhood trauma, including physical, sexual, or emotional abuse, is a well-documented predisposing factor. Such adverse experiences often disrupt psychological development and contribute to maladaptive coping mechanisms, increasing susceptibility to later binge-eating behaviors.
B. Restrictive dieting initiated during early life frequently serves as a precursor to disordered eating. Repeated cycles of dieting often trigger biological and psychological cravings, ultimately leading to loss-of-control eating episodes characteristic of this disorder.
D. Emotional dysregulation, specifically the inability to identify or manage negative affect, is a primary vulnerability factor. Patients frequently utilize food as a maladaptive strategy to soothe distress, reinforcing the cycle of binge-eating as an emotional coping mechanism.
E. A genetic predisposition is evident in the family history of mood disorders and substance use. These familial psychiatric patterns suggest a heritable component in the regulation of impulse control and neurobiological reward systems associated with binge-eating.
Rationale for incorrect answers:
C. Secure attachment, characterized by supportive and consistent caregiving, is actually a protective factor. This positive emotional environment fosters healthy regulatory skills and resilience, which typically decreases the likelihood of developing severe eating pathology or disordered eating behaviors.
Test-taking strategy:
Analyze the scenario/question: The question asks to identify established risk factors for the development of binge-eating disorder. This requires distinguishing between known psychological, developmental, and genetic vulnerabilities versus protective factors.
Apply knowledge of biopsychosocial risk factors: Evaluate each choice based on current psychiatric literature regarding the etiology of binge-eating disorder. Focus on how environmental, psychological, and genetic stressors increase vulnerability.
- Rule in Choice 1: Adverse childhood experiences significantly impact emotional regulation and self-esteem, increasing the risk for eating disorders.
- Rule in Choice 2: The diet-binge cycle is a classic pathway; restrictive behaviors often result in metabolic and psychological pressure to overeat.
- Rule out Choice 3: Secure attachment acts as a buffer against pathology, reducing the emotional vacuum that binge-eating often fills.
- Rule in Choice 4: Impaired emotional regulation is a hallmark of the binge-eating clinical profile, explaining the function of binging as an emotional stabilizer.
- Rule in Choice 5: Co-occurring family psychiatric history indicates shared genetic susceptibility for impulsive, mood-related, and addictive behaviors.
Take home points
- Childhood trauma is a significant psychological precursor for disordered eating development
- Restrictive dieting patterns often paradoxically increase the risk for subsequent loss-of-control binge episodes
- Deficits in emotional regulation are central to the behavioral pathology of binge-eating disorder
- Familial psychiatric history, including mood and substance use disorders, highlights the genetic/heritable risk
The nurse is reviewing the health record of a client with binge-eating disorder who has several comorbid conditions. Which of the following findings should the nurse address first?
No explanation
The nurse is explaining the neurobiological basis of binge-eating disorder to a nursing student. Which of the following best reflects the underlying pathophysiology?
Explanation
Binge-eating disorder often manifests alongside various physical comorbidities requiring comprehensive management. However, prioritizing care based on the client’s safety is the fundamental responsibility of the nursing professional during every assessment.
Rationale for correct answers:
A. Passive thoughts regarding the desire to end life necessitate immediate suicide risk assessment. Ensuring client safety is the highest clinical priority over all other medical findings, as immediate intervention is required to prevent self-harm.
Rationale for incorrect answers:
B. Hyperglycemic findings indicative of type 2 diabetes require long-term metabolic glucose management. While important for health maintenance, this condition is chronic and stable, and does not pose the immediate life-threatening risk associated with potential suicidal ideation.
C. Gastroesophageal reflux resulting from overeating requires symptomatic lifestyle modifications or medical intervention. This condition causes chronic discomfort but does not constitute an acute emergency that supersedes the urgent need for psychiatric safety evaluation and support.
D. Daytime sleepiness suggestive of obstructive sleep apnea warrants a referral for a sleep study and diagnostic evaluation. Although obstructive sleep apnea can lead to serious long-term cardiovascular consequences, it is currently stable and secondary to the immediate psychological safety concern.
Test-taking strategy:
Analyze the scenario/question: The question is a prioritization exercise requiring the nurse to identify the most urgent finding among several comorbidities in a client with binge-eating disorder.
Apply the ABCs and Priority Frameworks: Evaluate each finding using the principles of safety and stabilization. Prioritize life-threatening conditions (e.g., suicide risk) over chronic physical comorbidities (e.g., metabolic or respiratory issues).
- Rule in Choice 1: Suicidal ideation represents the highest level of risk; nursing priority is always to ensure the safety of the client first.
- Rule out Choice 2: Type 2 diabetes is a chronic metabolic condition that, while serious, does not require immediate, emergency nursing intervention in this context.
- Rule out Choice 3: Gastroesophageal reflux is a chronic discomfort that can be managed after the client's psychological safety is established.
- Rule out Choice 4: Obstructive sleep apnea is a chronic respiratory condition that requires long-term diagnosis and treatment planning rather than urgent intervention.
Take home points
- Client safety and suicide risk assessment take absolute priority over all physical comorbidities
- Chronic physical conditions such as diabetes and sleep apnea require ongoing management but are not immediate emergencies
- Prioritization in nursing is guided by the potential for imminent harm to the client
- Psychiatric symptoms must be assessed with the same urgency as acute physiological crises
Practice Questions 2
The nurse reviews the diagnostic criteria for binge-eating disorder. Which of the following, according to current standards, must be present for the diagnosis to be established?
Explanation
Binge-eating disorder is a recognized psychiatric diagnosis defined by specific, recurrent behavioral patterns. Establishing a formal diagnosis requires adherence to rigorous diagnostic criteria that differentiate this condition from other eating disorders and normative overeating.
Rationale for correct answers:
A. Frequency criteria require that binge-eating episodes occur on average at least once weekly for a duration of three months. This temporal threshold distinguishes significant pathology from isolated episodes of excessive consumption in the general population.
Rationale for incorrect answers:
B. Recurrent self-induced vomiting is a diagnostic criterion specific to bulimia nervosa, not binge-eating disorder. The absence of compensatory behaviors is actually a defining feature that helps clinicians rule out bulimia during the diagnostic assessment process.
C. A low body mass index below 18.5 kg/m² is a clinical indicator often associated with anorexia nervosa. Binge-eating disorder is typically associated with a range of weights, often including overweight or obesity, rather than the low weight thresholds seen in restrictive disorders.
D. Undue influence of body shape and weight on self-evaluation is a central diagnostic feature of anorexia nervosa and bulimia nervosa. While individuals with binge-eating disorder may experience body dissatisfaction, this specific cognitive distortion is not a formal requirement for the diagnosis.
Test-taking strategy:
Analyze the scenario/question: The question asks to identify the specific diagnostic requirement for binge-eating disorder according to established clinical standards.
Apply knowledge of diagnostic criteria: Evaluate each option against the criteria for binge-eating disorder versus other common eating disorders (e.g., anorexia nervosa, bulimia nervosa). Distinguish between behavior frequency, compensatory actions, and cognitive distortions.
- Rule in Choice 1: The frequency of at least one episode per week for three months is the mandatory quantitative threshold for this diagnosis.
- Rule out Choice 2: Compensatory purging behaviors define bulimia nervosa, which is a separate clinical entity from binge-eating disorder.
- Rule out Choice 3: Low body weight is a diagnostic hallmark of anorexia nervosa, whereas binge-eating disorder is not defined by a specific low body mass index.
- Rule out Choice 4: The extreme cognitive focus on body shape and weight as a self-worth determinant is characteristic of bulimia and anorexia, not the primary diagnostic criteria for binge-eating disorder.
Take home points
- Diagnosis of binge-eating disorder requires a minimum frequency of one episode per week for three months
- The absence of compensatory behaviors like purging is a critical factor for the diagnosis
- Weight status is not a diagnostic criteria for binge-eating disorder, unlike restrictive eating disorders
- Psychiatric diagnostic standards emphasize behavioral frequency over psychological preoccupation with body shape
The nurse documents that a client with binge-eating disorder reports an average of six binge episodes per week. Based on established severity specifiers, which of the following severity levels should the nurse recognize as correct?
Explanation
Binge-eating disorder severity is systematically categorized based on the weekly frequency of binge episodes. This classification enables clinicians to track treatment progress and determine the appropriate intensity of psychiatric and nutritional interventions for the individual client.
Rationale for correct answers:
B. Moderate severity is defined by a frequency of four to seven binge episodes per week. A report of six episodes per week correctly places the client within this specific diagnostic range of severity.
Rationale for incorrect answers:
A. Mild severity encompasses a frequency of one to three binge episodes per week. Because the client reports six episodes, this level is clinically underestimated based on the established diagnostic criteria for symptom frequency.
C. Severe severity is characterized by eight to thirteen binge episodes per week. The client’s reported frequency of six episodes does not meet this higher symptomatic threshold required for a severe classification.
D. Extreme severity is assigned when the client experiences fourteen or more binge episodes per week. This level represents the most frequent intensity of the disorder, which significantly exceeds the client's current reported frequency.
Test-taking strategy:
Analyze the scenario/question: The question requires determining the severity level of binge-eating disorder based on a specific frequency of six binge episodes per week.
Apply knowledge of severity specifiers: Review the recognized frequency thresholds used to categorize binge-eating disorder (Mild: 1–3, Moderate: 4–7, Severe: 8–13, Extreme: 14+). Map the client's reported frequency to these defined ranges.
- Rule out Choice 1: The client’s frequency of six exceeds the mild range of one to three episodes per week.
- Rule in Choice 2: Six episodes per week falls squarely within the established moderate range of four to seven episodes per week.
- Rule out Choice 3: The client’s frequency is below the threshold of eight, which is required for the severe classification.
- Rule out Choice 4: The frequency is significantly below the extreme threshold of fourteen or more episodes per week.
Take home points
- Severity for binge-eating disorder is categorized by the frequency of binge episodes per week
- Mild severity is defined by one to three episodes per week
- Moderate severity is defined by four to seven episodes per week
- Severe and extreme classifications apply to frequencies of eight or more episodes per week
The nurse assesses a client for behavioral and psychological features associated with binge-eating disorder. Which of the following findings would the nurse expect? Select all that apply
Explanation
Binge-eating disorder is characterized by specific pathological eating behaviors and associated psychological distress. Recognizing these manifestations is essential for accurate clinical diagnosis and for differentiating this condition from other disordered eating patterns or normal eating habits.
Rationale for correct answers:
A. Eating alone due to embarrassment is a hallmark behavioral indicator. Patients often hide the quantity of food consumed during an episode to avoid social judgment, reflecting the profound shame tied to their loss of control.
B. Eating rapidly until uncomfortably full is a primary behavioral feature. This rapid intake is often driven by an inability to regulate the pace of consumption, resulting in significant physical discomfort following the binge episode.
D. Negative emotions like disgust, depression, or guilt are expected psychological findings. These feelings typically manifest after an episode, reinforcing the cycle of distress and often triggering the next binge as a maladaptive coping mechanism.
Rationale for incorrect answers:
C. Compensatory fasting and meticulous calorie counting are diagnostic indicators of restrictive eating disorders or bulimia nervosa. These behaviors are contrary to the criteria for binge-eating disorder, which is defined by the absence of compensatory mechanisms to lose weight.
E. Structured eating without distress indicates normative, healthy behavior. By definition, binge-eating disorder involves significant impairment and distress, making the absence of anxiety or loss of control incompatible with this clinical diagnosis.
Test-taking strategy:
Analyze the scenario/question: The nurse is identifying behavioral and psychological indicators specific to binge-eating disorder. The objective is to select all findings that reflect the core symptoms of the disorder versus those that belong to other pathologies or normal function.
Apply knowledge of diagnostic behavioral patterns: Evaluate each choice against the DSM-5 criteria for binge-eating disorder, focusing on eating speed, social habits, post-episode emotions, and the presence or absence of compensation.
- Rule in Choice 1: Social isolation during binging is a common defensive behavior driven by intense embarrassment.
- Rule in Choice 2: Rapid consumption to the point of discomfort is a classic, objective behavioral sign of a binge.
- Rule out Choice 3: Calorie counting and compensatory fasting are deliberate, restrictive actions characteristic of anorexia or bulimia, not binge-eating disorder.
- Rule in Choice 4: Significant post-binge psychological distress is a mandatory diagnostic feature for this condition.
- Rule out Choice 5: A lack of distress and presence of structured eating are markers of healthy, non-pathological eating.
Take home points
- Binge-eating disorder is marked by eating rapidly and eating in secret due to shame
- Intense feelings of disgust, guilt, or depression are consistent psychological responses following a binge
- Compensatory behaviors such as fasting are not features of binge-eating disorder
- The diagnosis requires the presence of psychological distress and loss of control during eating episodes
The nurse evaluates a client with a long history of binge-eating disorder for physical complications. Which of the following findings should the nurse most anticipate as a consequence of the disorder?
Explanation
Binge-eating disorder is frequently associated with chronic metabolic complications due to recurrent cycles of overeating and resulting adiposity. Identifying these physical health impacts is critical for comprehensive care, as these patients often require proactive metabolic monitoring and long-term medical management of their physical comorbidities.
Rationale for correct answers:
B. Type 2 diabetes is a common physical complication linked to the obesity frequently observed in binge-eating disorder. The metabolic strain of excessive caloric intake and insulin resistance makes glucose regulation a primary health concern for this patient population.
Rationale for incorrect answers:
A. Dental erosion occurs in bulimia nervosa due to the acid exposure from repeated self-induced vomiting. This physical finding is not a consequence of binge-eating disorder, as it lacks the purging behaviors that cause gastric acid to damage oral structures.
C. Lanugo and bradycardia are classic physiological signs of severe malnutrition and starvation, which are diagnostic indicators of anorexia nervosa. These findings are inconsistent with the clinical presentation of binge-eating disorder, which does not involve starvation physiology.
D. Hypokalemia and electrolyte imbalances are dangerous consequences of chronic laxative misuse or purging. Since individuals with binge-eating disorder do not engage in these compensatory mechanisms, they are not at risk for the electrolyte derangements seen in bulimic patients.
Test-taking strategy:
Analyze the scenario/question: The nurse is tasked with identifying the physical complications most anticipated in a client with binge-eating disorder, specifically distinguishing them from the complications of other eating disorders.
Apply knowledge of eating disorder pathophysiology: Compare the physiological outcomes of binge-eating disorder (metabolic/obesity-related) with those of restrictive or purging disorders (malnutrition/electrolyte-related).
- Rule out Choice 1: Purging-related dental damage is specific to bulimia nervosa, not the binge-eating disorder profile.
- Rule in Choice 2: Obesity-related metabolic syndrome and diabetes are the hallmark physical complications of long-standing binge-eating disorder.
- Rule out Choice 3: Signs of starvation, such as lanugo and bradycardia, are clinical manifestations of anorexia nervosa, not binge-eating disorder.
- Rule out Choice 4: Laxative-induced hypokalemia is a specific complication of the purging behaviors seen in bulimia, which is absent in binge-eating disorder.
Take home points
- Binge-eating disorder is strongly associated with metabolic complications like type 2 diabetes
- Patients with binge-eating disorder do not typically exhibit the physical signs of purging
- Starvation-related symptoms are not characteristic of the binge-eating clinical profile
- Comprehensive physical assessment must focus on obesity-related comorbidities rather than malnutrition indicators
The nurse must differentiate binge-eating disorder from other conditions in a client who reports overeating during depressive episodes. Which of the following features should the nurse recognize as the priority distinguishing characteristic of binge-eating disorder?
Explanation
Binge-eating disorder is a distinct psychiatric condition defined by the presence of binge episodes characterized by an objective loss of control. While overeating can occur in other disorders, this specific psychological impairment distinguishes binge-eating from normative overeating or appetitive shifts associated with depressive syndromes.
Rationale for correct answers:
A. A subjective sense of loss of control is the defining diagnostic criterion for a binge episode. This internal experience differentiates the pathological binge from other forms of overeating, such as comfort eating or social consumption, where the individual remains in control of their intake.
Rationale for incorrect answers:
B. An increased appetite reported within a depressive syndrome, such as atypical depression, is not synonymous with a binge episode. This increased caloric intake generally lacks the rapid, out-of-control, and distress-inducing binge episodes required for a binge-eating disorder diagnosis.
C. The consumption of a large amount of food during social gatherings is a common behavioral occurrence that is usually not associated with a loss of control. Such consumption does not typically produce the distress or impaired functioning that characterizes a clinical binge episode.
D. Gradual weight gain is a common physical outcome of many behaviors, including dietary overconsumption or metabolic changes. This weight gain does not provide diagnostic information regarding the presence of binge-eating disorder, as it lacks the necessary focus on discrete, out-of-control eating behavior.
Test-taking strategy:
Analyze the scenario/question: The goal is to differentiate binge-eating disorder from other forms of overeating, specifically in the context of a client experiencing depressive symptoms.
Apply knowledge of diagnostic criteria: Focus on the defining characteristics of a clinical "binge" according to psychiatric standards. Distinguish between simple overeating or increased appetite and the specific psychological impairment of loss of control.
- Rule in Choice 1: The sense of being unable to stop or control what or how much one is eating is the hallmark of the disorder.
- Rule out Choice 2: Increased appetite in depression is an appetitive change, not a loss-of-control behavioral event.
- Rule out Choice 3: Eating large amounts in social settings is often normative and lacks the clinical markers of a pathological binge.
- Rule out Choice 4: Weight gain is a non-specific outcome and does not confirm the presence of binge-eating disorder behavior.
Take home points
- Binge-eating disorder is identified by a subjective loss of control during eating episodes
- Atypical depression can cause increased appetite but does not inherently involve pathological binge episodes
- Binge episodes must be distinguished from social overeating and general weight gain
- Diagnostic focus should always remain on the behavioral loss of control and the resulting psychological distress
Practice Questions 3
The nurse is interviewing a client suspected of having binge-eating disorder. Which of the following approaches would best facilitate accurate disclosure of the client's eating patterns?
Explanation
Therapeutic communication is essential when assessing patients with binge-eating disorder due to the significant stigma and shame surrounding the condition. Employing a nonjudgmental approach fosters a safe environment, which is vital for the patient to feel comfortable revealing the sensitive details of their eating patterns.
Rationale for correct answers:
B. A nonjudgmental, matter-of-fact manner minimizes the patient's fear of stigmatization. Because patients often harbor intense shame and embarrassment regarding their loss of control, this professional approach facilitates open disclosure and honest reporting of their binge episodes.
Rationale for incorrect answers:
A. Documenting the client's weight early in the interview can heighten anxiety and shame. For patients with eating disorders, focusing on physical metrics can feel judgmental and may cause the client to withdraw or minimize their reported behaviors.
C. Advising the client that dieting will resolve symptoms is counterproductive and medically inaccurate. Restrictive dieting is a known risk factor for triggering subsequent binge episodes; such advice undermines trust and demonstrates a lack of clinical understanding of the disorder.
D. Limiting questions to calorie counting is ineffective for diagnosing binge-eating disorder. The diagnosis is based on behavioral patterns, loss of control, and psychological distress, rather than specific numerical data which is often difficult for patients to accurately estimate or track.
Test-taking strategy:
Analyze the scenario/question: The nurse is determining the most effective communication strategy to elicit accurate information from a client suspected of having binge-eating disorder.
Apply therapeutic communication principles: Focus on strategies that reduce shame, build rapport, and gather diagnostic data regarding behaviors rather than metrics. Evaluate each option based on how it impacts the nurse-client relationship and data quality.
- Rule out Choice 1: Focusing on weight reinforces the patient's focus on shape and size, which often exacerbates the shame surrounding the disorder.
- Rule in Choice 2: Establishing a nonjudgmental, neutral tone is the gold standard for interviewing patients about sensitive psychiatric or behavioral health topics.
- Rule out Choice 3: This approach is dismissive of the complexity of the disorder and relies on harmful, incorrect interventions that exacerbate the binge-cycle.
- Rule out Choice 4: Calorie counting is not a diagnostic tool and does not capture the psychological experience of a binge episode.
Take home points
- Therapeutic rapport is the foundation for accurate assessment in eating disorder patients
- Stigma and shame are major barriers to disclosure that must be managed through neutral communication
- Dieting advice is contraindicated and can trigger worsening of binge-eating symptoms
- Assessment should focus on behavioral experiences, loss of control, and emotional distress rather than physical measurements
The nurse selects a validated instrument to screen a client for binge-eating disorder. Which of the following tools would be most appropriate for the nurse to use?
Explanation
Binge-eating disorder necessitates the use of validated screening instruments to accurately identify symptomatic patterns and facilitate early intervention. Selecting the correct diagnostic tool ensures that the nurse captures the specific behavioral and psychological data required to support a clinical evaluation.
Rationale for correct answers:
B. The Questionnaire on Eating and Weight Patterns is a validated screening tool specifically designed to assess for the presence of binge-eating disorder. It systematically evaluates the frequency of binge episodes, the experience of loss of control, and associated psychological distress.
Rationale for incorrect answers:
A. The Mini-Mental State Examination is used to assess cognitive impairment and neurological function. It is entirely unrelated to the assessment of eating behaviors or the diagnostic criteria specific to psychiatric eating pathologies.
C. The Glasgow Coma Scale is a clinical assessment utilized to evaluate the level of consciousness in patients with traumatic brain injury. This tool provides no information regarding behavioral habits or psychiatric concerns related to disordered eating.
D. The Hamilton Rating Scale for Depression is used to quantify the severity of depressive symptoms. While depressive comorbidities are common in binge-eating disorder, this scale does not screen for the specific diagnostic criteria or behaviors indicative of the eating disorder itself.
Test-taking strategy:
Analyze the scenario/question: The nurse needs to select a screening tool specifically validated for identifying the presence of binge-eating disorder. The task is to distinguish between general psychiatric/neurological assessments and specialized eating disorder screeners.
Apply knowledge of clinical assessment tools: Evaluate each tool by its intended clinical purpose. Only the tool designed for eating and weight patterns directly addresses the behavioral and symptomatic criteria for binge-eating disorder.
- Rule out Choice 1: Cognitive screening is irrelevant to the diagnosis of behavioral eating pathologies.
- Rule in Choice 2: This questionnaire is explicitly developed to screen for the presence of binge-eating disorder symptoms.
- Rule out Choice 3: Neurological status assessment is not applicable to the screening of psychiatric eating disorders.
- Rule out Choice 4: Depression scales assess mood, not the primary behavioral symptoms required to identify a binge-eating disorder diagnosis.
Take home points
- Specialized screening instruments are necessary for the accurate identification of binge-eating disorder
- The Questionnaire on Eating and Weight Patterns is a validated tool for identifying binge behavior
- Cognitive and neurological assessments like the MMSE and GCS have no role in eating disorder screening
- Mood-specific scales, while useful for comorbidity, do not screen for the eating disorder itself
The nurse is performing a physical assessment on a client with long-standing binge-eating disorder. Which of the following findings would the nurse expect to identify? Select all that apply
Explanation
Binge-eating disorder leads to significant metabolic complications due to recurrent cycles of overeating and chronic caloric surplus. Clinical assessment frequently reveals physical indicators of insulin resistance and cardiovascular strain, necessitating vigilant monitoring to prevent long-term systemic health consequences.
Rationale for correct answers:
A. A body mass index within the overweight or obese range is the most frequent physical finding. Chronic caloric excess often results in increased adipose tissue, which serves as a primary marker for the underlying metabolic imbalance.
B. Acanthosis nigricans, characterized by darkened, velvety skin, is a clinical manifestation of underlying insulin resistance. This finding is commonly observed in individuals with significant adiposity and elevated glucose levels, reflecting the metabolic impact of the disorder.
D. Elevated blood pressure is a frequent complication resulting from chronic obesity and systemic inflammation. Hypertension is an expected physiological finding that highlights the increased cardiovascular risk profile associated with long-term binge-eating behaviors.
Rationale for incorrect answers:
C. Parotid gland enlargement is a classic physical sign specifically associated with purging behaviors, such as self-induced vomiting. This clinical finding is absent in binge-eating disorder, as it lacks the recurrent purging pathology found in bulimia nervosa.
E. Lanugo is a fine, downy hair growth that develops as a protective physiological response to severe malnutrition and starvation. This finding is entirely inconsistent with the caloric surplus characteristic of binge-eating disorder and is instead diagnostic of anorexia nervosa.
Test-taking strategy:
Analyze the scenario/question: The nurse must identify physical examination findings consistent with the metabolic and physiological profile of binge-eating disorder, while excluding those characteristic of restrictive or purging eating disorders.
Apply knowledge of metabolic and physiological consequences: Contrast the physical presentation of binge-eating disorder (metabolic syndrome, obesity) with starvation or purging disorders (malnutrition, dental/glandular changes).
- Rule in Choice 1: Obesity is the most common physical correlate due to the sustained caloric excess inherent in the disorder.
- Rule in Choice 2: Signs of insulin resistance, such as acanthosis nigricans, are directly linked to the metabolic consequences of obesity.
- Rule out Choice 3: Parotid enlargement is a marker of repeated vomiting, which is not a component of binge-eating disorder.
- Rule in Choice 4: Hypertension is a common cardiovascular complication of obesity and metabolic strain in these clients.
- Rule out Choice 5: Lanugo is a marker of starvation and extreme caloric deficiency, which contradicts the diagnosis of binge-eating disorder.
Take home points
- Physical findings in binge-eating disorder typically reflect metabolic syndrome and obesity-related health complications
- Insulin resistance signs like acanthosis nigricans are clinically relevant in long-standing cases
- Purging-related signs such as parotid enlargement are not present in binge-eating disorder
- Starvation signs like lanugo are inconsistent with the overconsumption profile of the disorder
The nurse completes a psychosocial and mental status assessment of a client with binge-eating disorder. Which of the following findings should the nurse prioritize for further evaluation?
Explanation
Binge-eating disorder is frequently accompanied by significant psychological distress and comorbid psychiatric symptoms. Prioritizing care requires the nurse to identify and address the most acute safety risks to the client's life before focusing on behavioral symptoms or long-standing body image concerns.
Rationale for correct answers:
A. Passive thoughts of not wanting to wake up are high-risk indicators of potential suicidal ideation. Ensuring client safety is the absolute nursing priority, and this finding mandates immediate formal assessment to determine the presence of active suicidal intent or plan.
Rationale for incorrect answers:
B. Feeling embarrassed about eating alone is a symptomatic behavior consistent with the shame typical of binge-eating disorder. While this warrants therapeutic support and intervention, it is a psychological feature of the disorder and not an acute, life-threatening emergency.
C. Body dissatisfaction regarding shape and weight is a prevalent cognitive distortion among individuals with eating disorders. Although these feelings contribute to the client's psychological burden and warrant ongoing counseling, they do not require the same immediate intervention as potential self-harm.
D. Binge episodes triggered by stressful events illustrate the functional use of food as a maladaptive coping mechanism. This connection is essential for the client's long-term therapeutic success and symptom management but does not represent a critical threat to the client’s physical safety.
Test-taking strategy:
Analyze the scenario/question: The question asks the nurse to prioritize findings from a psychosocial assessment for a client with binge-eating disorder. The task is to distinguish between psychiatric symptoms associated with the eating disorder and an immediate risk to patient safety.
Apply the nursing process and safety principles: Prioritize assessment findings by the severity of potential harm. Use the hierarchy of needs to evaluate which finding necessitates the most urgent intervention.
- Rule in Choice 1: Suicidal ideation is a life-threatening psychiatric emergency that takes precedence over all other clinical findings.
- Rule out Choice 2: Shame and embarrassment are core emotional features of the disorder but are not acute emergencies.
- Rule out Choice 3: Cognitive distortions related to body image are chronic aspects of the pathology that require long-term behavioral treatment.
- Rule out Choice 4: Stress-triggered eating is a behavioral pattern that is a focus of the psychotherapy plan, not an immediate crisis.
Take home points
- Suicide risk assessment is the paramount priority in all psychiatric and behavioral assessments
- Emotional distress and shame are diagnostic components of the disorder but are managed after ensuring safety
- Behavioral triggers are important clinical findings for long-term psychotherapy planning
- Prioritization in nursing remains steadfastly centered on the principle of preventing self-harm and ensuring stability
The nurse reviews the laboratory results of a client with binge-eating disorder before pharmacologic therapy is initiated. Which of the following findings would the nurse most expect to identify as a complication of the disorder?
Explanation
Binge-eating disorder is profoundly linked to metabolic dysfunction resulting from chronic caloric surplus and systemic insulin resistance. Monitoring laboratory markers allows the nurse to identify the specific physiological consequences of the disorder, enabling safe initiation of pharmacological therapy aimed at symptom control.
Rationale for correct answers:
B. A glycated hemoglobin (HbA1c) of 7.4 percent indicates suboptimal glucose control consistent with a diagnosis of type 2 diabetes mellitus. This finding is an anticipated metabolic complication in clients with long-standing binge-eating disorder and associated adiposity.
Rationale for incorrect answers:
A. Hypokalemia (2.8 mEq/L) is a life-threatening electrolyte imbalance typically caused by chronic purging, such as self-induced vomiting or laxative abuse. This finding is not an expected consequence of binge-eating disorder, which lacks compensatory purging mechanisms.
C. Serum amylase elevation is frequently associated with repeated self-induced vomiting, as the parotid glands release higher enzyme levels into the circulation. Since binge-eating disorder does not involve purging, this elevation would not be expected in this clinical profile.
D. Hyponatremia (128 mEq/L) is an acute electrolyte disturbance that can result from over-hydration or specific purging behaviors. It is not a characteristic complication of binge-eating disorder and would represent an acute medical emergency unrelated to the disorder's primary metabolic profile.
Test-taking strategy:
Analyze the scenario/question: The question requires identifying the laboratory finding that most directly reflects the metabolic consequences of long-standing binge-eating disorder. The task is to distinguish between findings indicative of metabolic syndrome/diabetes versus those indicative of purging or acute instability.
Apply knowledge of physiological consequences: Contrast the metabolic impacts of overconsumption (e.g., hyperglycemia) with the physiological impacts of purging (e.g., electrolyte imbalance, elevated amylase).
- Rule out Choice 1: Hypokalemia is a specific marker of purging/malnutrition; it is not a feature of binge-eating disorder.
- Rule in Choice 2: Elevated HbA1c is a clinical marker for the metabolic syndrome frequently seen as a complication of untreated binge-eating disorder.
- Rule out Choice 3: Elevated amylase is a classic sign of parotid irritation due to frequent purging, which is absent in this diagnosis.
- Rule out Choice 4: Significant hyponatremia is not an expected clinical finding of binge-eating disorder and requires urgent investigation for other etiologies.
Take home points
- Metabolic complications, particularly type 2 diabetes, are highly prevalent in binge-eating disorder
- Laboratory findings in binge-eating disorder focus on glucose regulation and systemic metabolic health
- Purging-related indicators like hypokalemia and elevated amylase must be absent for a diagnosis
- Pharmacologic initiation requires baseline screening of metabolic parameters to ensure patient safety
Practice Questions 4
The nurse is formulating nursing diagnoses for a client newly admitted with binge-eating disorder and multiple comorbidities. Which of the following diagnoses should the nurse prioritize?
Explanation
Binge-eating disorder is associated with severe psychological comorbidities, necessitating a nursing approach that prioritizes immediate life safety. Identifying and addressing the most critical nursing diagnosis ensures that the psychiatric safety of the patient remains the paramount concern during the initial phases of admission.
Rationale for correct answers:
A. Risk for suicide is the priority diagnosis because it represents an immediate threat to the patient's survival. Although other diagnoses are highly relevant to the clinical picture of this disorder, nursing interventions must always prioritize the prevention of life-threatening outcomes over behavioral or psychological symptoms.
Rationale for incorrect answers:
B. Imbalanced nutrition, specifically intake exceeding requirements, is a primary behavioral consequence of recurrent binge episodes. While this diagnosis addresses the physical pathology of the disorder and requires comprehensive nutritional management, it does not supersede the urgency of evaluating and mitigating immediate suicidal risk.
C. Disturbed body image describes a cognitive and emotional reaction to the self, often rooted in societal pressures. This diagnosis is essential for the long-term therapeutic planning and cognitive-behavioral treatment of the client but lacks the acute safety urgency required for prioritization.
D. Chronic low self-esteem is a pervasive psychological burden frequently experienced by individuals struggling with the shame of eating disorders. This diagnosis is a critical focus for ongoing counseling and psychosocial intervention, but it is not an immediate clinical emergency compared to the potential for self-harm.
Test-taking strategy:
Analyze the scenario/question: The nurse is prioritizing nursing diagnoses for a client with a complex presentation of binge-eating disorder and psychiatric comorbidities. The goal is to identify the diagnosis that requires the most immediate intervention based on safety principles.
Apply the nursing process and safety hierarchy: Evaluate the urgency of each nursing diagnosis using Maslow’s hierarchy of needs and established safety protocols. Prioritize survival and safety above physical, emotional, or self-esteem needs.
- Rule in Choice 1: Suicidal risk is the highest priority diagnosis, requiring immediate stabilization and safety measures.
- Rule out Choice 2: Nutritional imbalances, while a central problem of the disorder, are chronic in nature and do not pose an immediate threat to life compared to suicidality.
- Rule out Choice 3: Body image disturbance is a psychological symptom that requires intensive, but not emergent, therapeutic management.
- Rule out Choice 4: Self-esteem deficits are common comorbidities that will be addressed throughout the comprehensive care plan but are not life-threatening.
Take home points
- The nursing process dictates that safety-related diagnoses always take precedence over behavioral or psychosocial ones
- Suicide risk is a frequent, life-threatening complication of eating disorders and mood comorbidities
- Behavioral diagnoses such as imbalanced nutrition require systemic management, including nutritional counseling and symptom tracking
- Prioritization ensures that the most critical threats to patient stability are addressed before chronic psychological concerns
The nurse is establishing outcome goals with a client who has binge-eating disorder. Which of the following outcomes reflects the most appropriate primary focus of care?
Explanation
Binge-eating disorder treatment success is best measured by the reduction of maladaptive behavioral frequency and the improvement of the patient's relationship with food. Prioritizing behavioral modification over rapid weight loss or restrictive practices ensures the patient achieves sustainable health outcomes while minimizing the risk of relapse.
Rationale for correct answers:
B. A measurable reduction in binge episodes is the most critical outcome, as it indicates the patient is gaining control over their eating patterns. This behavioral change directly reflects improved affective regulation and the efficacy of the therapeutic strategies implemented during treatment.
Rationale for incorrect answers:
A. Setting a goal for a specific body mass index within one month is unrealistic and psychologically damaging. Rapid weight loss goals often trigger compensatory dietary restriction, which paradoxically increases the risk for further loss-of-control binge episodes.
C. Adherence to a strict calorie-restricted meal plan is contraindicated in the treatment of binge-eating disorder. Rigid dieting schedules are known triggers for the binge cycle, as they impose excessive physiological and psychological pressure that the patient is currently working to manage.
D. Avoiding all high-carbohydrate foods is an unsustainable and restrictive practice that promotes "all-or-nothing" thinking patterns. This approach is detrimental to recovery, as it fails to address the underlying psychological triggers and fosters an unhealthy, avoidance-based relationship with nutrition.
Test-taking strategy:
Analyze the scenario/question: The nurse is establishing realistic and therapeutic outcome goals for a client with binge-eating disorder. The objective is to identify the goal that promotes sustainable recovery rather than dangerous, restrictive practices.
Apply evidence-based recovery principles: Evaluate each goal against the established standards for eating disorder recovery, which emphasize behavioral stability and psychological health over weight metrics or food avoidance.
- Rule out Choice 1: Rapid weight loss metrics are not primary clinical outcomes and can trigger relapse.
- Rule in Choice 2: Reducing the frequency of binge episodes is the primary behavioral target of treatment for this condition.
- Rule out Choice 3: Strict caloric restriction is a behavioral trigger for binge episodes and is contrary to recovery-oriented nutritional care.
- Rule out Choice 4: Restrictive elimination of food groups reinforces pathological eating patterns and increases cognitive distress.
Take home points
- Treatment success in binge-eating disorder is measured by behavioral stability and decreased frequency of episodes
- Rapid weight loss targets are inappropriate and potentially dangerous
- Avoidance of strict dietary restrictions is necessary to prevent triggering the binge-restrict cycle
- Outcome goals must be focused on psychological and behavioral health rather than physical aesthetics or weight
The nurse is planning nutritional interventions for a client with binge-eating disorder. Which of the following actions should the nurse include? Select all that apply
Explanation
Binge-eating disorder treatment requires nutritional rehabilitation that focuses on restoring regular, balanced intake and enhancing the client's connection to internal physiological cues. By abandoning restrictive practices and fostering a predictable meal structure, the client reduces the biological and emotional pressures that drive episodic overconsumption.
Rationale for correct answers:
A. Collaboration with a registered dietitian is essential for normalizing eating patterns through evidence-based nutritional support. This team approach ensures that the client receives structured, personalized guidance that balances nutritional requirements without triggering maladaptive behaviors.
B. Establishing regular meals and planned snacks is a core intervention to prevent biological and psychological deprivation. Predictable intake schedules help regulate metabolism and decrease the extreme hunger that often serves as a powerful trigger for binge episodes.
E. Assisting the client to distinguish physiological hunger from emotional cues is a critical cognitive-behavioral skill. This awareness allows the client to identify when food is being used for emotional soothing, facilitating the adoption of healthier, non-food coping mechanisms.
Rationale for incorrect answers:
C. Encouraging prolonged fasting is contraindicated, as it reinforces the restrictive aspect of the binge-restrict cycle. Fasting inevitably leads to profound hunger, which increases the likelihood of a subsequent binge due to the intense physiological need for energy.
D. Prescribing a rigid low-calorie diet is highly detrimental to recovery. Extreme restriction induces both metabolic and psychological stress, which acts as a major catalyst for relapse into binge episodes and deepens the client's experience of shame.
Test-taking strategy:
Analyze the scenario/question: The goal is to identify appropriate nutritional interventions that align with established treatment protocols for binge-eating disorder, focusing on normalization rather than restriction.
Apply principles of nutritional rehabilitation: Select interventions that foster regularity and mindfulness while ruling out those that reinforce restrictive patterns or promote weight-focused pathology.
- Rule in Choice 1: Professional collaboration is necessary for holistic care and normalization of eating.
- Rule in Choice 2: Regular, consistent intake is the most effective biological defense against binge triggers.
- Rule out Choice 3: Fasting is a restrictive behavior that triggers future binge episodes.
- Rule out Choice 4: Rigid dieting is a hallmark trigger that increases the risk of loss-of-control eating.
- Rule in Choice 5: Mindfulness and body-cue awareness are fundamental skills for managing emotional overeating.
Take home points
- Nutritional rehabilitation prioritizes consistent, regular eating patterns over weight loss
- Dieting and fasting are harmful practices that perpetuate the binge-eating cycle
- Interdisciplinary collaboration with dietitians is essential for successful symptom management
- Developing the ability to differentiate physiological hunger from emotional triggers is a key recovery goal
The nurse in an outpatient setting is establishing a therapeutic relationship with a client who has binge-eating disorder. Which of the following nursing approaches would be most therapeutic?
Explanation
Binge-eating disorder is defined by a cycle of behavioral loss-of-control and profound psychological pain. Establishing a therapeutic relationship predicated on empathy and acceptance is the foundational step in treating this condition, as it directly counteracts the pervasive feelings of shame and secrecy that often lead patients to isolate themselves and avoid seeking essential care.
Rationale for correct answers:
A. A nonjudgmental attitude is the most therapeutic approach because it creates a safe environment for the patient to discuss their eating patterns without fear of stigmatization. By reducing the shame and secrecy that surround binge episodes, the nurse encourages the patient to engage openly, which is essential for accurate assessment and effective clinical intervention.
Rationale for incorrect answers:
B. Emphasizing that the client is responsible for controlling their behavior is counterproductive and harmful. This approach ignores the neurobiological and psychiatric aspects of the disorder, serving only to reinforce the patient's existing self-blame and failure, which exacerbates the cycle of distress and binge-eating.
C. Focusing discussions on body weight is highly contraindicated in the treatment of binge-eating disorder. This focus reinforces the patient's pathological preoccupation with their size, increases their anxiety, and distracts from the core therapeutic objective of achieving behavioral stability and emotional health.
D. Advising the client to conceal their disorder from family is unethical and medically inappropriate. Healthy recovery requires the development of a support system; encouraging secrecy further isolates the client and prevents the involvement of family members who could otherwise play a vital role in the patient's long-term recovery and stability.
Test-taking strategy:
Analyze the scenario/question: The goal is to identify the most therapeutic nursing intervention for building a rapport with a client suffering from binge-eating disorder. The task is to prioritize empathetic, evidence-based practices that foster recovery while ruling out shame-inducing or harmful advice.
Apply principles of therapeutic communication: Evaluate each approach based on its capacity to build trust, reduce pathology-related shame, and facilitate openness within the nurse-client relationship.
- Rule in Choice 1: Empathy and a non-judgmental stance are essential components of nursing practice for psychiatric and behavioral health.
- Rule out Choice 2: Blaming the patient for lack of control is judgmental and ignores the complex psychiatric nature of the diagnosis.
- Rule out Choice 3: Focusing on weight reinforces the patient's core cognitive distortions and increases the risk of relapse.
- Rule out Choice 4: Promoting secrecy is damaging to the client’s support system and is contrary to the goal of holistic, integrated care.
Take home points
- The therapeutic relationship is based on unconditional positive regard and the reduction of patient shame
- Shifting the focus away from weight is essential to breaking the cycle of disordered eating
- Promoting open communication with family members can enhance the client's support network
- Blaming the client for their symptoms is detrimental to the clinical outcomes and the therapeutic process
Study Guide: Therapeutic Relationship in Binge-Eating Disorder
- Core Therapeutic Tasks: Build trust, validate the patient's emotional distress, and normalize the need for professional help.
- Addressing Shame: Explicitly communicate that binge-eating disorder is a clinical condition, not a personal failing or lack of willpower.
- Focus Areas: Discuss behavioral triggers, coping mechanisms, and emotional regulation rather than weight, caloric counts, or willpower.
- Professional Boundaries: Maintain a supportive yet professional stance that encourages the client to take an active, informed role in their own recovery journey.
The nurse is teaching a client with binge-eating disorder to use behavioral and cognitive strategies. Which of the following instructions would be most appropriate for the nurse to include?
Explanation
Binge-eating disorder treatment utilizes cognitive behavioral strategies to increase patient self-awareness and foster healthier emotional regulation. By documenting thoughts, feelings, and behavioral patterns, the client develops the necessary insights to interrupt the binge cycle and replace maladaptive habits with sustainable coping mechanisms.
Rationale for correct answers:
A. A food and mood diary is a fundamental cognitive tool that helps the client identify specific environmental, emotional, and physical binge triggers. This reflective process allows the patient to recognize the relationship between distress and overeating, which is essential for developing effective prevention strategies.
Rationale for incorrect answers:
B. Skipping meals is a restrictive behavior that paradoxically intensifies hunger and psychological deprivation. This compensatory practice is a primary driver of the binge-restrict cycle; therefore, it is directly opposed to the goal of establishing consistent, balanced nutritional habits.
C. Frequent weighing reinforces a hyper-fixation on body size and weight fluctuations. This behavior significantly increases anxiety and self-criticism, which often serves as a trigger for further episodes of binge-eating rather than promoting progress or stability.
D. Avoiding all social situations involving food is socially isolating and impractical for long-term recovery. Instead of total avoidance, therapy should focus on developing adaptive skills to manage social interactions and cultivate a healthy, neutral relationship with communal dining.
Test-taking strategy:
Analyze the scenario/question: The nurse is educating a client on evidence-based cognitive and behavioral strategies for managing binge-eating disorder. The task is to identify the intervention that promotes self-awareness and regulation while avoiding common maladaptive traps.
Apply principles of cognitive-behavioral therapy: Evaluate each strategy based on its ability to enhance insight and stability without reinforcing the disordered cycle of restriction or preoccupation.
- Rule in Choice 1: Self-monitoring through diaries is a gold-standard behavioral technique for identifying triggers in binge-eating disorder.
- Rule out Choice 2: Compensatory restriction (skipping meals) is a dangerous behavior that reinforces the pathology of the disorder.
- Rule out Choice 3: Repeated daily weighing exacerbates cognitive distortions and increases the risk of relapse.
- Rule out Choice 4: Avoidance strategies are unsustainable and fail to address the underlying psychological challenges inherent in social eating.
Take home points
- Self-monitoring tools like food and mood diaries are critical for identifying behavioral triggers
- Restrictive behaviors such as skipping meals are contraindicated and trigger the binge-restrict cycle
- Monitoring body weight too frequently increases psychological distress and anxiety
- Social avoidance is an unhelpful coping strategy; the focus should be on developing adaptive social skills
Practice Questions 5
The nurse is reviewing psychotherapy options for clients with binge-eating disorder. Which of the following modalities have demonstrated effectiveness in reducing binge behavior? Select all that apply
Explanation
Psychotherapeutic modalities are central to managing binge-eating disorder by addressing underlying maladaptive patterns and improving emotional regulation. Evidence-based interventions prioritize behavioral stability, social functioning, and the modulation of distress to decrease the frequency of binge episodes.
Rationale for correct answers:
A. Cognitive-behavioral therapy effectively targets irrational dietary rules and negative cognitive distortions. This structured approach helps patients identify triggers, modify eating patterns, and challenge beliefs that sustain the cycle of binge behavior and persistent shame.
C. Dialectical behavior therapy provides essential skills for improving emotion regulation and distress tolerance. By teaching mindfulness and interpersonal effectiveness, this modality reduces the tendency to utilize food as a maladaptive mechanism to cope with intense, overwhelming affective states.
E. Interpersonal psychotherapy improves outcomes by specifically addressing relational difficulties and social functioning. This approach helps the client resolve interpersonal disputes and transitions, which are often significant emotional stressors that precipitate binge-eating episodes in vulnerable individuals.
Rationale for incorrect answers:
B. Aversion therapy utilizes noxious stimuli and is generally considered unethical and ineffective for treating eating disorders. This outdated approach does not address the psychological complexity of binge-eating and may cause harm by reinforcing shame and fear rather than promoting healthy regulation.
D. Insight-oriented psychoanalysis focuses on childhood conflicts and does not prioritize current behavioral change. This modality has limited empirical support for reducing binge behavior and is rarely utilized as a first-line treatment for the immediate management of this disorder.
Test-taking strategy:
Analyze the scenario/question: The nurse is identifying effective psychotherapeutic treatments for binge-eating disorder. The objective is to select evidence-based modalities while ruling out obsolete or ineffective methods.
Apply knowledge of psychotherapeutic evidence: Evaluate each option based on established psychiatric literature regarding binge-eating disorder. Focus on treatments that foster behavioral change and emotional stability versus those that focus on deep archetypal analysis or archaic punishment.
- Rule in Choice 1: Cognitive-behavioral therapy is the gold standard for binge-eating disorder management due to its focus on behavior and thought patterns.
- Rule out Choice 2: Aversion therapy is clinically discredited and is not an accepted, ethical practice for treating eating disorders.
- Rule in Choice 3: Dialectical behavior therapy is highly effective for clients who experience significant emotional dysregulation during binge episodes.
- Rule out Choice 4: Psychoanalysis is too slow and lacks specific evidence for reducing binge frequency compared to structured cognitive therapies.
- Rule in Choice 5: Interpersonal psychotherapy is recognized as an effective treatment by addressing interpersonal contributors to the patient's distress.
Take home points
- Cognitive-behavioral therapy is the primary evidence-based treatment for binge-eating disorder
- Dialectical behavior therapy helps clients manage the emotional dysregulation that triggers binges
- Interpersonal psychotherapy targets relational stressors that contribute to disordered eating patterns
- Aversion therapy and pure psychoanalysis are not recommended treatments for binge-eating disorder
The nurse is providing medication teaching to a client with binge-eating disorder and comorbid depression who has been prescribed a selective serotonin reuptake inhibitor. Which of the following statements should the nurse include?
Explanation
Selective serotonin reuptake inhibitors (SSRIs) are frequently utilized in the management of binge-eating disorder and comorbid depressive symptoms to enhance mood and reduce behavioral impulsivity. These agents primarily act by increasing synaptic serotonin availability, which necessitates a consistent dosing schedule to achieve the therapeutic neurochemical stabilization required for long-term symptom management.
Rationale for correct answer:
A. Therapeutic efficacy with SSRIs requires consistent administration to achieve the biochemical changes necessary for mood improvement. It is a critical teaching point that patients should not expect immediate relief, as these medications typically require four to six weeks of steady use to reach their full clinical impact.
Rationale for incorrect answers:
B. Discontinuation syndrome is a significant risk when antidepressants are stopped abruptly without medical supervision. Patients must be taught that even if mood improves, they must continue the regimen to maintain neurological stability and prevent the sudden return of depressive or binge-related symptoms.
C. Weight loss is not a primary or immediate pharmacological outcome of SSRI therapy. These agents do not function as appetite suppressants, and the patient must be cautioned against unrealistic expectations regarding physical changes, which could otherwise trigger further maladaptive eating behaviors.
D. Consistent dosing is essential for maintaining therapeutic blood levels of the medication. Taking the medication only on an intermittent, "as-needed" basis is ineffective for managing mood or eating patterns and significantly undermines the physiological goal of achieving sustained neurotransmitter modulation.
Test-taking strategy:
Analyze the scenario/question: The client is starting an SSRI for binge-eating disorder and depression. The goal is to identify safe, accurate educational information regarding antidepressant adherence, timeline, and expectations.
Apply knowledge of SSRI pharmacology: Evaluate each statement based on standard antidepressant teaching principles (time to effect, adherence, mechanism of action, and expected outcomes).
- Rule in Choice 1: The delayed onset of therapeutic action is a fundamental concept in antidepressant education to prevent early discontinuation.
- Rule out Choice 2: Abrupt cessation of SSRIs can lead to adverse withdrawal effects and relapse, making this advice unsafe.
- Rule out Choice 3: SSRIs are not indicated for weight loss, and focusing on this metric can trigger cognitive distortions about body shape.
- Rule out Choice 4: SSRIs require steady-state plasma concentrations for efficacy; they are not PRN (as-needed) medications for acute binge episodes.
Take home points
- SSRIs require a consistent daily dosing schedule to maintain therapeutic efficacy
- Therapeutic benefits, including improved mood, typically require several weeks of continuous use
- Discontinuation should only occur under medical supervision to avoid withdrawal symptoms
- Antidepressants are not weight-loss medications and should not be presented as such to patients
The nurse in an interdisciplinary team is coordinating care for a client with binge-eating disorder. Which of the following clients should the nurse prioritize for placement in an inpatient level of care?
Explanation
Inpatient level of care for binge-eating disorder is mandated by clinical conditions that threaten immediate safety or physiological homeostasis. Prioritizing care requires the nurse to distinguish between patients who can manage their condition in the community and those whose acute medical instability or psychiatric risk necessitates twenty-four-hour observation and multidisciplinary intervention.
Rationale for correct answer:
A. Medical instability combined with active suicidal ideation constitutes a critical emergency. This client requires immediate admission to a secure, inpatient unit to ensure physical safety, facilitate intensive psychiatric stabilization, and manage physiological complications that cannot be safely treated in an outpatient or community setting.
Rationale for incorrect answers:
B. Moderate symptoms occurring within the context of a supportive home environment allow for safe and effective management in an outpatient program. This patient does not meet the acuity criteria for inpatient hospitalization, as they have access to external resources and a safe, stable support structure.
C. A referral request for an outpatient dietitian indicates the patient is actively engaging in their own recovery and is stable enough to pursue community-based support. This request is a positive behavioral sign and demonstrates the client's capacity to utilize lower levels of care.
D. Occasional binge episodes managed with self-help demonstrate a baseline of stability and personal autonomy. This client is currently utilizing self-management tools successfully, which suggests that the clinical risk is low and does not warrant the high-intensity environment of an inpatient facility.
Test-taking strategy:
Analyze the scenario/question: The nurse is applying principles of care coordination and triage to determine the appropriate level of treatment for various clients. The task is to prioritize the client with the highest acuity and safety risk.
Apply the principles of triage and acuity: Evaluate each client based on the severity of their psychiatric and medical presentation. Prioritize those who are currently "unstable" or "high-risk" for self-harm, as these represent emergencies that bypass standard elective care.
- Rule in Choice 1: Suicidality and medical instability are the primary indicators for immediate inpatient psychiatric admission.
- Rule out Choice 2: Home stability and moderate symptoms are classic indicators that an outpatient or partial-hospitalization program is appropriate.
- Rule out Choice 3: This client is demonstrating self-advocacy and is stable enough to engage with outpatient services.
- Rule out Choice 4: Successful self-help indicates a low level of acuity and does not necessitate inpatient care.
Take home points
- Inpatient admission is reserved for patients who are medically or psychiatrically unstable
- Suicidal ideation with intent or plan is a psychiatric emergency requiring immediate secure placement
- Stable home environments and personal capacity for self-care support outpatient treatment success
- Triage decisions are based on objective assessments of risk, stability, and available support systems
The nurse is evaluating the prognosis of a client treated for binge-eating disorder. Which of the following factors is most associated with a favorable outcome?
Explanation
Binge-eating disorder necessitates comprehensive treatment involving cognitive behavioral therapy and pharmacotherapy to address psychological patterns and prevent further metabolic complications associated with recurrent episodes of uncontrolled overconsumption of food.
Rationale for correct answer:
B. Early intervention facilitates prompt engagement with multidisciplinary care, improving long-term prognosis for clients. Sustained adherence to a structured therapeutic plan minimizes the risk of physical comorbidities and emotional distress while promoting stable eating behaviors.
Rationale for incorrect answers:
A. Delayed treatment often allows the disorder to become deeply ingrained, significantly complicating the recovery process. Prolonged patterns of uncontrolled eating increase the likelihood of severe metabolic syndrome and associated chronic health issues before clinical support is initiated.
C. Restrictive dieting frequently triggers a cycle of deprivation that leads to further episodes of compulsive binging. This maladaptive behavior prevents the development of healthy nutritional habits and maintains the underlying psychological distress driving the disorder.
D. Ongoing follow-up is essential to monitor for potential relapse triggers throughout the recovery journey. Discontinuing care prematurely often leads to the resurgence of dysfunctional behaviors once environmental or emotional stressors reappear in the client's life.
Test-taking strategy:
Analyze the scenario/question: The question asks for the most significant predictor of a positive clinical outcome for a client with binge-eating disorder, requiring the identification of factors that foster sustainable recovery versus those that maintain psychopathology.
Apply knowledge of therapeutic models: Recovery from eating disorders requires a multifaceted approach that addresses both behavioral patterns and underlying psychological triggers. Successful management is inherently linked to early detection and the commitment to a long-term, comprehensive therapeutic framework.
- Rule out Choice 1: Delaying care exacerbates the condition, making long-term resolution much more difficult to achieve.
- Rule in Choice 2: Early, consistent, and comprehensive care is the gold standard for achieving lasting remission and healthier behaviors.
- Rule out Choice 3: Restrictive dieting is a known pathological trigger for binge-eating cycles, not a solution for recovery.
- Rule out Choice 4: Consistent long-term monitoring is necessary to prevent relapse and support continued psychological stability.
Take home points
- Early initiation of comprehensive treatment is the primary predictor of a favorable prognosis in binge-eating disorder.
- Restrictive dieting must be avoided as it reinforces the cycle of binge-eating and psychological distress.
- Ongoing follow-up is critical even after initial stabilization to manage potential relapse triggers.
- Multidisciplinary interventions including therapy and nutrition education are superior to isolated attempts at weight control.
The nurse is caring for a client with binge-eating disorder who has capacity to make decisions but declines a recommended treatment. Which of the following ethical principles should the nurse most uphold in this situation?
Explanation
Ethical principles guide clinical practice by balancing the individual rights of patients with the professional duty to provide care, emphasizing that competent decision-making must remain protected within the healthcare environment.
Rationale for correct answer:
A. Autonomy recognizes that the client maintains the fundamental right to accept or refuse any proposed medical intervention. Respecting this principle ensures that care remains centered on the patient's informed choices regardless of the professional recommendation.
Rationale for incorrect answers:
B. Beneficence involves acting in the best interest of the patient, but it does not supersede autonomy when the patient possesses decision-making capacity. Forcing treatment against a competent client's wishes violates their personal liberty and rights.
C. Justice focuses on the fair and equitable distribution of healthcare resources across populations. While important in organizational policy, it is not the primary principle governing an individual client's right to decline specific treatments.
D. Nonmaleficence means the duty to do no harm, which requires transparent communication of risks. Withholding information is a violation of ethics and standard practice, as it undermines the client's ability to provide informed consent.
Test-taking strategy:
Analyze the scenario/question: The scenario involves a client with the mental capacity to make decisions who is refusing a treatment recommendation. The question asks to identify the governing ethical principle that protects this refusal.
Apply knowledge of bioethical principles: Nursing practice is grounded in four major pillars: autonomy, beneficence, nonmaleficence, and justice. When a client is competent, autonomy is generally prioritized over the other principles to ensure the client retains control over their body and medical path.
- Rule in Choice 1: Autonomy is the governing principle that upholds the client's capacity for self-determination.
- Rule out Choice 2: Beneficence cannot be used to justify overriding the expressed wishes of a competent adult client.
- Rule out Choice 3: Justice relates to resource allocation and social equity, which is unrelated to individual treatment refusal.
- Rule out Choice 4: Nonmaleficence demands transparency, so withholding information would be considered unethical conduct.
Take home points
- Autonomy is the cornerstone of ethical nursing practice when dealing with competent clients.
- Competent adults have the legal and ethical right to refuse any medical treatment.
- Beneficence does not justify overriding the rights of a competent patient.
- Informed consent requires full disclosure of risks and benefits, not the withholding of information.
Comprehensive Questions
The nurse is describing binge-eating disorder to a group of nursing students. Which of the following statements best captures the essential feature of a binge episode?
Explanation
Binge-eating disorder is characterized by recurrent episodes of consumption of excessive amounts of food, accompanied by a subjective sense of losing control over the intake during these events.
Rationale for correct answer:
A. Loss of control over eating is the pathognomonic feature defining a true binge episode. Clients often feel unable to stop eating or limit the quantity of food consumed during these distressing clinical events.
Rationale for incorrect answers:
B. Self-induced vomiting is a hallmark behavior seen in bulimia nervosa, rather than binge-eating disorder. The absence of recurrent inappropriate compensatory behaviors is a key diagnostic criterion used to differentiate these conditions.
C. Small amounts of food consumption do not meet the clinical criteria for a binge episode. Eating while experiencing anxiety about weight is a common psychological comorbid symptom but does not constitute a binge episode.
D. Physiological hunger is a normal response to energy deficits and is not indicative of disordered eating. Binge episodes typically occur in the absence of hunger, driven by emotional or psychological triggers rather than biological necessity.
Test-taking strategy:
Analyze the scenario/question: The question requires identifying the primary diagnostic criterion for a binge episode in binge-eating disorder, necessitating a clear understanding of what distinguishes this disorder from other eating pathologies like bulimia nervosa.
Apply knowledge of diagnostic criteria: Binge-eating disorder is formally defined in the DSM-5 by the presence of recurrent binge-eating episodes occurring at least once a week for three months, characterized by eating larger than normal amounts of food within a discrete period and experiencing a sense of lack of control, without regular compensatory behaviors.
- Rule in Choice 1: Loss of control is the essential diagnostic component distinguishing binge episodes.
- Rule out Choice 2: Compensatory behaviors like induced vomiting characterize bulimia nervosa, not binge-eating disorder.
- Rule out Choice 3: Eating small amounts represents a restrictive pattern, which contradicts the definition of a binge.
- Rule out Choice 4: Eating only during physiological hunger is a healthy behavior and the opposite of a binge episode.
Take home points
- Binge-eating disorder is defined by episodes of excessive consumption and a loss of control.
- Absence of regular compensatory behaviors like purging differentiates this disorder from bulimia nervosa.
- Binge episodes are often driven by emotional dysregulation rather than true physiological hunger.
- Diagnostic criteria require the binge episodes to occur at least weekly for three months.
The nurse is reviewing the historical classification of binge-eating disorder. Which of the following statements accurately reflects its diagnostic status?
Explanation
Binge-eating disorder underwent significant clinical refinement before gaining recognition as a distinct psychiatric diagnosis within the DSM-5, reflecting its unique morbidity and specialized evidence-based treatment requirements.
Rationale for correct answer:
A. Formal recognition as an independent condition was achieved in the DSM-5. This change established specific criteria that differentiate the disorder from other eating pathologies based on clinical presentation and diagnostic history.
Rationale for incorrect answers:
B. Anorexia nervosa has a distinct diagnostic history separate from binge-eating disorder. The two conditions have historically been classified independently due to their unique physiological, psychological, and behavioral diagnostic characteristics.
C. Provisional status is no longer applicable to this disorder since its official inclusion. It is currently a fully established diagnosis within the psychiatric manual, supported by extensive research and validation.
D. Bulimia nervosa is a distinct condition characterized by compensatory behaviors. Binge-eating disorder was previously considered an unspecified eating disorder but is now defined as a separate entity from bulimia nervosa.
Test-taking strategy:
Analyze the scenario/question: The question assesses knowledge of the psychiatric diagnostic history regarding binge-eating disorder, requiring the distinction between its former status as a research category and its current status as an independent diagnosis.
Apply knowledge of psychiatric history: Understanding the evolution of the DSM (Diagnostic and Statistical Manual of Mental Disorders) is essential for nursing students. Binge-eating disorder was included in the DSM-IV as a category for further study and was upgraded to a formal, standalone diagnosis in the DSM-5, which was published in 2013 to better capture the clinical needs of these clients.
- Rule in Choice 1: The transition to a formal diagnosis occurred explicitly with the release of the DSM-5.
- Rule out Choice 2: Anorexia nervosa has been a distinct category for much longer, making this historical claim inaccurate.
- Rule out Choice 3: Binge-eating disorder is a confirmed diagnosis, not a provisional category under current standards.
- Rule out Choice 4: It is a standalone diagnosis and is not classified as a subtype of bulimia.
Take home points
- Binge-eating disorder was promoted to an official, independent diagnosis in the DSM-5.
- The diagnostic distinction is crucial because it helps identify clients who do not engage in purging behaviors.
- Historical context is important for understanding the evolution of psychiatric care and research.
- The classification change reflects the clinical consensus on the disorder's severity and unique profile.
The nurse is teaching about the prevalence of eating disorders. Which of the following statements about binge-eating disorder should the nurse include?
Explanation
Binge-eating disorder has emerged as the most prevalent eating disorder in the United States, affecting individuals across diverse demographics and necessitating increased awareness of its significant public health implications.
Rationale for correct answer:
D. Prevalence data confirms that this condition is the most common eating disorder among adults. It affects a broader segment of the population than anorexia or bulimia due to its wide-ranging demographic distribution.
Rationale for incorrect answers:
A. Gender distribution for this disorder is much more balanced than other eating conditions. Research indicates that the ratio is far closer to 1.5:1 rather than the highly skewed ratios seen in other diagnoses.
B. Adult populations are frequently affected, and the disorder is not restricted by age. Clinical evidence shows that onset can occur during young adulthood or midlife, persisting well into the later stages of life.
C. Overweight status and obesity are highly prevalent comorbidities in clients with this disorder. In fact, many individuals seeking treatment for weight-related issues meet the diagnostic criteria for this specific psychiatric condition.
Test-taking strategy:
Analyze the scenario/question: The question asks to identify the most accurate epidemiological statement regarding the prevalence and distribution of binge-eating disorder, requiring the differentiation of clinical facts from common misconceptions about eating disorders.
Apply knowledge of epidemiology: When analyzing prevalence, it is critical to understand that binge-eating disorder differs from anorexia nervosa and bulimia nervosa in its gender parity and its strong association with excess weight. Recognizing these epidemiological distinctions helps in correctly identifying the disorder's status as a major public health concern.
- Rule out Choice 1: The gender disparity is significantly less pronounced than in other disorders, making the 20:1 ratio factually incorrect.
- Rule out Choice 2: The condition is clearly documented in adult populations, contradicting the claim that it is limited to adolescents.
- Rule out Choice 3: There is a strong, established clinical correlation between this disorder and elevated body mass index (BMI).
- Rule in Choice 4: Large-scale surveys consistently identify this as the most frequently reported eating disorder in the general population.
Take home points
- Binge-eating disorder is the most common eating disorder in the general population.
- The prevalence shows a more balanced gender distribution compared to other eating disorders.
- The condition frequently coexists with overweight or obesity, making it a critical screening focus.
- Onset and prevalence span across all age groups, not just adolescents.
The nurse is identifying protective factors that reduce vulnerability to binge-eating disorder. Which of the following should the nurse recognize as protective? Select all that apply
Explanation
Protective factors function by fostering psychological resilience and healthy behavioral habits that shield individuals from developing maladaptive eating patterns, thereby mitigating the developmental risk of binge-eating disorder.
Rationale for correct answers:
A. Secure attachment provides a stable emotional foundation that promotes healthy self-esteem. Supportive family environments facilitate the development of resilient personality traits and effective communication, which significantly decrease vulnerability to psychiatric disorders.
B. Emotion-regulation strategies empower individuals to manage stress and distress without resorting to maladaptive coping mechanisms. Developing these skills is essential for maintaining psychological stability and reducing reliance on food as a primary emotional coping tool.
D. Structured eating patterns help maintain metabolic balance and prevent the physiological triggers associated with hunger-induced binging. Establishing a consistent, healthy relationship with food is a fundamental behavioral defense against disordered eating.
Rationale for incorrect answers:
C. Restrictive dieting acts as a major risk factor rather than a protective one, as it fosters a cycle of deprivation and compulsive overconsumption. Chronic limitation of food intake is a recognized precursor to triggering binge episodes.
E. Internalizing ideals regarding body shape, such as the thin ideal, increases susceptibility to body dissatisfaction and negative self-evaluation. This cultural pressure frequently drives individuals toward dangerous weight-control methods that perpetuate disordered eating cycles.
Test-taking strategy:
Analyze the scenario/question: The question asks for protective factors that decrease the risk of binge-eating disorder, requiring the identification of positive psychological and behavioral health indicators as opposed to established risk factors.
Apply knowledge of eating disorder etiology: Risk reduction involves identifying environmental and psychological elements that support healthy self-image and behavioral regulation. Protective factors generally include strong support systems and healthy stress-management techniques, whereas factors that promote body dissatisfaction or behavioral volatility (like dieting) serve as risk amplifiers.
- Rule in Choice 1: Strong relational bonds and secure attachment reduce vulnerability to emotional disturbances.
- Rule in Choice 2: The ability to regulate emotions serves as a primary defense against disordered eating behaviors.
- Rule out Choice 3: Dieting is a well-established precursor that drives cycles of disordered eating.
- Rule in Choice 4: Consistent, balanced eating prevents the metabolic instability that often triggers binges.
- Rule out Choice 5: Internalizing unrealistic body ideals increases psychological distress and body dissatisfaction.
Take home points
- Protective factors for binge-eating disorder include psychological, familial, and behavioral stability.
- Secure relationships and effective emotional coping skills build resilience against psychiatric illness.
- Restrictive dieting is a major risk factor and should be discouraged to prevent disordered eating.
- Internalization of thinness ideals is a negative factor that increases body dissatisfaction and disorder risk.
The nurse is caring for a client with binge-eating disorder who has several coexisting conditions. Which of the following is the most common psychiatric comorbidity the nurse should anticipate?
Explanation
Major depressive disorder represents the most prevalent psychiatric comorbidity found in individuals diagnosed with binge-eating disorder, significantly impacting the clinical course, symptom severity, and overall psychological well-being of affected clients.
Rationale for correct answer:
C. Major depression frequently presents alongside this disorder, as both conditions are deeply linked by shared emotional dysregulation and negative self-appraisal. This clinical connection often requires integrated care to effectively manage the depressive symptoms while addressing the disordered eating behaviors.
Rationale for incorrect answers:
A. Schizophrenia is a severe chronic psychiatric condition that is not commonly associated with binge-eating disorder. The etiology and clinical presentation of psychotic disorders differ vastly from the behavioral and psychological dynamics of eating pathologies.
B. Dissociative identity disorder is a rare condition characterized by fragmented consciousness. It is not an anticipated or typical comorbidity observed in the clinical management of clients presenting with binge-eating patterns.
D. Obsessive-compulsive disorder shares some features of behavioral repetition, yet it is significantly less prevalent in this population than depressive disorders. While anxiety is often present, depression is the most frequently diagnosed comorbid condition in this specific patient demographic.
Test-taking strategy:
Analyze the scenario/question: The question requires identifying the most common psychiatric comorbidity associated with binge-eating disorder, necessitating an understanding of the epidemiological overlap between eating disorders and mood disorders.
Apply knowledge of psychiatric comorbidities: Binge-eating disorder is rarely an isolated condition. Clinicians must screen for mood and anxiety disorders, as they frequently co-occur and exacerbate the cycle of binging. Understanding that major depression is the most statistically significant co-occurring condition helps the nurse prioritize screenings and interventions.
- Rule in Choice 3: Depression is the most prevalent psychiatric condition found in patients with binge-eating disorder.
- Rule out Choice 1: Schizophrenia is statistically uncommon in this population and does not share a high correlation with binging.
- Rule out Choice 2: Dissociative identity disorder is a rare disorder that is not clinically linked to the prevalence of binge-eating disorder.
- Rule out Choice 4: Although anxiety can occur, major depression remains the most frequent diagnosis observed in these clinical settings.
Take home points
- Major depressive disorder is the most frequent comorbid psychiatric condition seen in clients with binge-eating disorder.
- Integrated assessment for both mood and eating disorders is essential for comprehensive care planning.
- Understanding the connection between emotional distress and binge episodes is vital for effective nursing intervention.
- Screening for depression should be a standard component of the psychiatric evaluation for patients with eating pathologies.
The nurse is explaining the neurobiology of binge-eating disorder. Which of the following neurotransmitter systems is most implicated in the reward dysregulation of the disorder?
Explanation
Neurobiological research consistently identifies reward dysregulation as a central component of binge-eating disorder, focusing on the mesolimbic pathways that mediate reinforcement, craving, and the compulsive repetition of food-seeking behaviors.
Rationale for correct answer:
B. Dopamine pathways within the mesolimbic system are responsible for the reinforcing effects of high-calorie foods. Dysregulation here often leads to diminished baseline signaling, prompting individuals to engage in binge episodes to achieve a temporary neurochemical reward.
Rationale for incorrect answers:
A. Glutamatergic system activity within the cerebellum primarily regulates motor coordination and fine movement. It lacks a direct role in the hedonic evaluation or the reinforcement mechanisms that drive the pathological binging cycle.
C. Cholinergic system activity in the basal forebrain is primarily involved in arousal, attention, and cognitive function. It does not play a primary role in the specific reward-seeking behaviors associated with eating disorders.
D. Histaminergic system function within the tuberomammillary nucleus is crucial for the regulation of the sleep-wake cycle and alertness. It is not implicated in the neuropsychiatric basis of reward-driven overconsumption or impulsive behavior.
Test-taking strategy:
Analyze the scenario/question: The question requires identifying the specific neurobiological system involved in the reward-processing deficits of binge-eating disorder, necessitating an understanding of how brain pathways influence compulsive behavior.
Apply knowledge of neurobiology: The mesolimbic dopamine system, often called the brain's "reward circuit," is the primary focus of research regarding addiction and binge-type eating. When dopamine signaling is impaired or dysregulated, individuals may struggle to feel satisfied by normal intake, leading to compensatory overconsumption.
- Rule in Choice 2: Dopamine is the key neurotransmitter mediating the reward, motivation, and reinforcement loop in binge-eating disorder.
- Rule out Choice 1: The cerebellar glutamatergic system is involved in motor control and is not the primary site for reward-based behavioral pathology.
- Rule out Choice 3: The cholinergic system handles arousal and attention, which are not the mechanisms driving the binge-eating cycle.
- Rule out Choice 4: The histaminergic system is dedicated to alertness and wakefulness, which does not influence the reinforcement of binge behaviors.
Take home points
- The mesolimbic dopamine system is the primary neurobiological pathway involved in reward dysregulation.
- Binge-eating disorder involves a dysfunction in how the brain perceives and responds to the hedonic reward of food.
- Diminished dopamine receptor sensitivity may contribute to the need for larger quantities of food to achieve satisfaction.
- Neurobiological findings support treating binge-eating disorder with mechanisms that address reward and impulsivity.
The nurse is discussing the heritability of binge-eating disorder with a client whose relatives are affected. Which of the following statements is most accurate for the nurse to make?
Explanation
Genetic research indicates that binge-eating disorder involves complex interactions between familial transmission and environmental factors, establishing a clear heritable basis for the condition beyond just individual lifestyle choices.
Rationale for correct answer:
B. Twin studies and family aggregation research strongly support that genetic predisposition plays a major role in the development of the disorder. Heritability estimates demonstrate that biology significantly influences one's vulnerability to these eating behaviors.
Rationale for incorrect answers:
A. Inheritance patterns for psychiatric conditions are polygenic and multifactorial, not dictated by a single parent's diagnosis. The disorder may manifest in individuals without any direct parental history due to diverse contributing variables.
C. Multifactorial etiology means that biology and genetics interact with environmental stressors to trigger the illness. Attributing the disorder strictly to personal choices ignores the well-documented biological and genetic underpinnings.
D. Family history is a recognized risk factor for developing the disorder, as familial aggregation studies show increased prevalence among biological relatives. Ignoring this connection minimizes the critical role of heredity in pathogenesis.
Test-taking strategy:
Analyze the scenario/question: The question asks for the most accurate statement regarding the heritability and etiology of binge-eating disorder, requiring the student to identify the balance between genetics and environmental factors in psychiatric conditions.
Apply knowledge of complex genetics: Most psychiatric and eating disorders are not caused by a single gene or a single parent's history; rather, they result from the interplay of polygenic inheritance and environmental triggers. Acknowledging a significant familial component is clinically accurate and helps reduce the stigma often associated with attributing disorders solely to lifestyle failures.
- Rule out Choice 1: The disorder does not follow simple Mendelian patterns; it does not require a parental diagnosis to manifest.
- Rule in Choice 2: Scientific evidence identifies a significant genetic and familial contribution to the disorder's development.
- Rule out Choice 3: Reducing the condition to personal choice ignores the substantial influence of biological vulnerability and complex environmental triggers.
- Rule out Choice 4: Heredity is a major factor, and studies confirm it is not unrelated to family history.
Take home points
- Binge-eating disorder is a complex psychiatric condition with significant genetic and familial components.
- Genetic predisposition interacts with environmental triggers to determine susceptibility to the disorder.
- There is no single gene or mandatory parental history required for the development of the condition.
- Attribution of the disorder to personal lifestyle choices is scientifically inaccurate and stigmatizing.
The nurse is assessing the psychological triggers of a client's binge episodes. Which of the following findings would the nurse most expect to identify?
Explanation
Binge-eating disorder is a psychiatric condition characterized by the use of food as a maladaptive mechanism to manage negative affect or intense psychological distress rather than to satisfy caloric requirements.
Rationale for correct answer:
A. Negative affect frequently precedes binge episodes as clients utilize compulsive eating to temporarily numb feelings of sadness or anxiety. These emotional states act as primary psychological triggers for the loss of control observed during these behavioral events.
Rationale for incorrect answers:
B. Contentment periods are typically associated with stable mood states and adaptive eating behaviors. Binge episodes are driven by maladaptive coping strategies aimed at relieving emotional pain or severe psychological discomfort rather than existing in a state of wellness.
C. Physiological hunger is a homeostatic signal that directs healthy intake, whereas binge episodes operate independently of satiety signals. These events are primarily driven by neurological reinforcement and emotional dysregulation rather than the biological necessity of caloric replenishment.
D. Feelings of pride are inconsistent with the phenomenology of binge-eating disorder, which is characterized by profound post-binge shame and emotional suffering. These episodes inevitably result in psychological distress and a decline in self-esteem following the conclusion of the event.
Test-taking strategy:
Analyze the scenario/question: The question requires identifying the emotional precursors to binge episodes, necessitating the differentiation between healthy eating motivations and the pathological drivers of binge-eating disorder.
Apply knowledge of emotional dysregulation: Binge-eating disorder is categorized by the use of food for emotional regulation. The "binge-eating cycle" typically begins with an emotional trigger, leading to a period of uncontrolled eating that provides temporary emotional relief, followed by intense shame and guilt, which subsequently lowers self-esteem and increases the likelihood of future binging.
- Rule in Choice 1: Emotional distress is the primary psychological driver for compulsive overconsumption.
- Rule out Choice 2: Episodes are not motivated by positive affect or general contentment states.
- Rule out Choice 3: Binges are distinct from normal appetite or hunger-based eating patterns.
- Rule out Choice 4: Bingeing is associated with guilt and shame rather than feelings of achievement or pride.
Take home points
- Binge episodes in binge-eating disorder are driven by negative emotions rather than physiological hunger.
- Psychological triggers such as anxiety, sadness, and stress are the most common precursors to binge events.
- The aftermath of a binge episode is characterized by profound emotional distress, shame, and guilt.
- Treatment focuses on developing adaptive coping skills to manage emotions without relying on maladaptive food consumption.
The nurse is teaching about sociocultural contributors to binge-eating disorder. Which of the following should the nurse identify as relevant factors? Select all that apply
Explanation
Sociocultural factors play a foundational role in the pathogenesis of eating disorders by reinforcing maladaptive perceptions of body shape and influencing the behavioral patterns that trigger pathological binge episodes.
Rationale for correct answers:
A. Thin ideal internalization drives body dissatisfaction and the adoption of extreme weight-control behaviors. This cultural pressure fosters negative self-evaluation, which serves as a psychological precursor to the loss of control observed in binge episodes.
B. Weight stigmatization and experiences of teasing create significant psychological stress and emotional vulnerability. This chronic social devaluation promotes shame, anxiety, and low self-worth, which clients frequently attempt to mitigate through compulsive food consumption.
C. Food restriction creates a cycle of biological deprivation and psychological tension that eventually necessitates an overcompensatory response. Chronic dieting is a behavioral catalyst that undermines physiological hunger signals and directly triggers the onset of pathological bingeing.
Rationale for incorrect answers:
D. Family meals that are structured and supportive serve as a protective barrier against eating disorders. This environment fosters healthy habits and nutritional balance, which are incompatible with the development of disordered eating behaviors.
E. Positive image is a strong psychological buffer that protects individuals against societal pressures and thinness ideals. High self-esteem functions as a resilient foundation, reducing the likelihood that an individual will succumb to maladaptive dieting or emotional bingeing.
Test-taking strategy:
Analyze the scenario/question: The question requires identifying sociocultural and behavioral contributors to the development of binge-eating disorder, necessitating a clear distinction between factors that exacerbate vulnerability and those that provide protection.
Apply knowledge of eating disorder etiology: The development of binge-eating disorder is a multifactorial process where sociocultural pressures (like the media-promoted thin ideal and stigma) interact with behavioral habits (like restrictive dieting). By identifying these elements, the nurse can recognize the environmental and personal pressures that increase a client's susceptibility to disordered eating.
- Rule in Choice 1: The internalization of the thin ideal is a major sociocultural trigger for body dissatisfaction.
- Rule in Choice 2: Experiencing weight-based stigma is a harmful social stressor that perpetuates disordered eating.
- Rule in Choice 3: Rigid dieting and restriction are primary behavioral drivers that induce the binge-cycle.
- Rule out Choice 4: Regular family meals are a protective environment that promotes nutritional stability.
- Rule out Choice 5: High self-esteem is a resilient psychological trait that guards against disordered eating.
Take home points
- Sociocultural influences such as media-promoted ideals and weight stigma are major contributors to the disorder's development.
- Chronic dieting and food restriction are behavioral precursors that fundamentally disrupt the binge-eating cycle.
- Supportive family environments and positive self-regard act as protective factors against disordered eating.
- Clinical interventions must address both internal psychological factors and external sociocultural pressures to be effective.
The nurse is verifying the diagnostic frequency threshold for binge-eating disorder. Which of the following must be met for the diagnosis?
Explanation
Binge-eating disorder is defined by specific diagnostic frequency criteria that ensure the identified behavior represents a persistent and clinically significant pattern rather than an isolated or infrequent event.
Rationale for correct answer:
D. Diagnostic criteria establish that binge episodes must occur on average at least once weekly for a duration of at least three months. This threshold distinguishes the pathological disorder from occasional, non-disordered overconsumption of food.
Rationale for incorrect answers:
A. Twice daily frequency far exceeds the clinical threshold required for the diagnosis. While this frequency indicates severe pathology, the formal criterion only mandates a minimum of once weekly for the specified time period.
B. Once monthly is an insufficient frequency to meet the diagnostic requirements for the disorder. The criteria necessitate a more consistent pattern of behavior over the designated period to justify a clinical diagnosis.
C. Stressful events are often triggers, but they are not the sole context for the diagnosis. Binge eating must meet the established frequency regardless of the specific external stressors or emotional triggers identified by the client.
Test-taking strategy:
Analyze the scenario/question: The question asks for the specific diagnostic threshold required to formally identify binge-eating disorder, requiring knowledge of the DSM-5 criteria concerning the frequency and duration of binge episodes.
Apply knowledge of diagnostic standards: Nurses must differentiate between occasional episodes of overeating and the clinical disorder. The DSM-5 criteria are clear: the binge episodes must occur at least once a week for at least three consecutive months. This timeframe and frequency help confirm that the disorder is a persistent behavioral pattern.
- Rule out Choice 1: A frequency of twice daily is far more frequent than the minimum required for the diagnosis.
- Rule out Choice 2: A frequency of once per month is too infrequent to meet the established clinical standard.
- Rule out Choice 3: The diagnosis is based on behavioral frequency, not the circumstantial nature of the triggers.
- Rule in Choice 4: The threshold of at least once weekly for three months is the mandatory clinical requirement.
Take home points
- Binge-eating disorder is defined by specific frequency and duration criteria in the DSM-5.
- The mandatory diagnostic threshold is a minimum of one binge episode per week for at least three months.
- Understanding these criteria helps differentiate the disorder from occasional instances of overeating.
- Clinical diagnosis requires consistent behavioral patterns rather than isolated or infrequent episodes.
Study Guide: Diagnostic Thresholds for Binge-Eating Disorder
- Diagnostic Manual: Formal criteria are outlined in the Diagnostic and Statistical Manual of Mental Disorders (DSM-5).
- Timeframe: Symptoms must persist for a minimum of three months to reach the diagnostic threshold.
- Frequency Requirement: A minimum average frequency of one binge episode per week is required for a formal diagnosis.
- Clinical Significance: The episodes must be accompanied by distress, loss of control, and specific behavioral markers, not just the frequency of eating.
- Diagnostic Utility: These strict criteria prevent the over-diagnosis of the disorder while ensuring that individuals experiencing clinically significant pathology receive appropriate care.
The nurse documents that a client experiences an average of ten binge episodes per week. Which of the following severity specifiers should the nurse assign?
Explanation
Binge-eating disorder severity is determined by the weekly frequency of binge episodes, allowing clinicians to tailor the therapeutic intensity required to address the client's specific clinical needs and behavioral symptoms.
Rationale for correct answer:
C. Severe classification applies when the client reports an average of eight to thirteen binge episodes per week. This specific range of behavioral frequency necessitates intensive intervention to prevent further physical complications and to support long-term clinical stabilization.
Rationale for incorrect answers:
A. Mild severity is assigned when there are one to three episodes per week. Ten episodes per week significantly exceeds this clinical threshold, meaning a mild classification would underestimate the intensity of the patient's symptoms.
B. Moderate severity applies to a range of four to seven episodes per week. Because the patient reports ten episodes, this classification is insufficiently descriptive of the higher frequency of the pathological behavior observed in this clinical case.
D. Extreme severity is reserved for an average of fourteen or more episodes per week. While the patient’s behavior is clinically significant, it has not yet reached the frequency criteria required for the highest level of diagnostic severity classification.
Test-taking strategy:
Analyze the scenario/question: The question asks to assign a severity specifier for binge-eating disorder based on a reported frequency of ten episodes per week, requiring knowledge of the DSM-5 severity classification scale.
Apply knowledge of severity specifiers: Clinical severity is categorized by the average number of binge episodes per week: Mild (one to three), Moderate (four to seven), Severe (eight to thirteen), and Extreme (fourteen or more). This standardized scale allows for consistent assessment and documentation of the disorder's progression and treatment response.
- Rule out Choice 1: Mild severity is restricted to a lower range of one to three weekly episodes.
- Rule out Choice 2: Moderate severity covers the range of four to seven weekly episodes only.
- Rule in Choice 3: Ten episodes per week falls directly within the eight to thirteen range defined for severe cases.
- Rule out Choice 4: Extreme severity begins at fourteen or more weekly episodes.
Take home points
- Severity specifiers in binge-eating disorder are based on the average weekly frequency of binge episodes.
- Standardized ranges are: Mild (one to three), Moderate (four to seven), Severe (eight to thirteen), and Extreme (fourteen or more).
- Accurate documentation of frequency is essential for determining appropriate treatment intensity and level of care.
- These specifiers provide a consistent clinical metric to track a client's improvement or regression during therapy.
The nurse is differentiating binge-eating disorder from bulimia nervosa. Which of the following features is unique to bulimia nervosa?
Explanation
Bulimia nervosa is a distinct psychiatric diagnosis distinguished from binge-eating disorder by the consistent application of inappropriate compensatory behaviors used to prevent weight gain after episodes of excessive food intake.
Rationale for correct answer:
C. Compensatory behaviors such as self-induced vomiting, laxative abuse, or excessive exercise are the defining features that differentiate bulimia nervosa from binge-eating disorder. These actions are used to manage the caloric impact of binge consumption and are absent in the clinical definition of binge-eating disorder.
Rationale for incorrect answers:
A. Loss of control is a shared characteristic observed in both binge-eating disorder and bulimia nervosa. It represents a core behavioral symptom that reflects the inability to regulate intake during a discrete binge event.
B. Large amounts of food consumption during a discrete period is a diagnostic requirement for both conditions. Both disorders involve this excessive intake as a primary component of the binge-eating episode itself.
D. Marked distress regarding the eating behavior is experienced by individuals suffering from both conditions. This emotional reaction is a common clinical finding across various eating disorders and does not serve as a differentiating feature.
Test-taking strategy:
Analyze the scenario/question: The question requires identifying the primary clinical feature that distinguishes bulimia nervosa from binge-eating disorder, focusing on the specific behavioral markers defined in the DSM-5.
Apply knowledge of diagnostic criteria: Differentiating between eating disorders is critical for determining the correct therapeutic approach. While the binge episodes themselves may appear similar in terms of quantity and loss of control, the presence or absence of compensatory purging is the clear diagnostic line.
- Rule out Choice 1: Loss of control is a shared diagnostic symptom in both conditions.
- Rule out Choice 2: Consuming large quantities of food is a common diagnostic criterion for both disorders.
- Rule in Choice 3: Recurrent compensatory behaviors like purging or exercise are unique to bulimia nervosa.
- Rule out Choice 4: Clinical distress is a universal psychological feature of all major eating disorders.
Take home points
- Bulimia nervosa is differentiated from binge-eating disorder by the presence of regular compensatory behaviors.
- Both disorders share core symptoms, including loss of control and the consumption of excessive food amounts.
- Understanding the diagnostic distinction is necessary for planning safe and effective psychiatric interventions.
- Compensatory behaviors in bulimia nervosa may include self-induced vomiting, misuse of laxatives, or extreme exercise.
The nurse is assessing a client for behavioral features of binge-eating disorder. Which of the following behaviors would the nurse expect? Select all that apply
Explanation
Binge-eating disorder entails specific behavioral patterns characterized by rapid consumption and secretive ingestion of food in the absence of physical hunger, reflecting an intense psychological drive to consume food despite satiety.
Rationale for correct answers:
A. Rapid eating is a classic behavioral sign of a binge episode, as clients often feel unable to slow down or control their pace. This speed of intake is a hallmark of the overwhelming urgency characterizing pathological bingeing.
B. Secretive eating behaviors, including the concealment of wrappers, are driven by the profound shame and guilt associated with the disorder. These actions are defensive measures used by clients to hide their loss of control from others.
C. Eating without hunger clearly distinguishes a binge episode from normal intake. Binge episodes are motivated by emotional dysregulation rather than the biological necessity of caloric intake, often occurring when the individual is already physically satiated.
Rationale for incorrect answers:
D. Self-induced vomiting is a compensatory behavior that defines bulimia nervosa, not binge-eating disorder. The absence of purging is a diagnostic requirement for distinguishing binge-eating disorder from other related pathological eating conditions.
5. Structured meal plans are indicative of recovery-oriented behavior or healthy eating patterns. The disorder is characterized by the complete disruption of structured eating, making strict adherence to a plan contrary to the symptomatic presentation observed.
Test-taking strategy:
Analyze the scenario/question: The question requires identifying the behavioral indicators that typify binge-eating disorder, necessitating the differentiation of binge-related actions from compensatory or healthy eating behaviors.
Apply knowledge of diagnostic behavioral signs: Binge-eating disorder is defined by specific behaviors occurring during the binge, such as eating much more rapidly than normal, eating until uncomfortably full, eating large amounts when not hungry, and eating alone due to embarrassment. These behavioral cues provide a clinical window into the loss of control and the emotional weight of the condition.
- Rule in Choice 1: Rapid intake is a primary behavioral marker of a binge episode.
- Rule in Choice 2: Secrecy is a common defensive behavior rooted in the intense shame of the disorder.
- Rule in Choice 3: Binging often occurs in the absence of physiological hunger, driven by emotional needs.
- Rule out Choice 4: Purging behaviors like vomiting are diagnostic exclusionary criteria for binge-eating disorder.
- Rule out Choice 5: Structured eating is the exact opposite of the impulsive and disorganized behavior found in binge-eating disorder.
Take home points
- Behavioral signs of binge-eating disorder include eating rapidly, secretive consumption, and eating despite the absence of hunger.
- Shame-driven behaviors, such as hiding evidence of bingeing, are common clinical findings.
- Purging behaviors like self-induced vomiting are not part of the clinical profile of binge-eating disorder.
- Recognizing these behaviors is essential for screening and early clinical intervention.
The nurse is evaluating a client with long-standing binge-eating disorder for physical complications. Which of the following is the client most at risk of developing?
Explanation
Binge-eating disorder is a metabolic health concern, where recurrent cycles of excessive caloric intake significantly increase the risk for long-term chronic diseases and inflammatory metabolic derangements.
Rationale for correct answer:
C. Metabolic syndrome and type 2 diabetes are frequent complications of the sustained caloric surplus associated with binge-eating disorder. The chronic nature of the pathological intake causes significant insulin resistance, leading to impaired glucose regulation and weight-related health risks.
Rationale for incorrect answers:
A. Lanugo and severe electrolyte depletion are classic complications of starvation-based eating disorders like anorexia nervosa. These physical findings result from prolonged nutritional insufficiency and purging, which are not present in individuals suffering from binge-eating disorder.
B. Enamel erosion is a hallmark sign of chronic purging through self-induced vomiting. Because binge-eating disorder does not involve the repeated exposure of teeth to gastric acid, clients do not typically exhibit these oral manifestations of bulimia.
D. Cachexia and amenorrhea are severe clinical consequences of significant underweight status and nutritional deprivation. These symptoms are clinically inconsistent with the presentation of binge-eating disorder, which is more commonly associated with overweight or obesity and caloric excess.
Test-taking strategy:
Analyze the scenario/question: The question requires identifying the physical health complications most associated with binge-eating disorder, necessitating a differentiation between the metabolic risks of overconsumption and the starvation/purging-based complications of other eating disorders.
Apply knowledge of pathophysiology: Binge-eating disorder is characterized by caloric excess, which leads to metabolic stress. Therefore, the nurse should anticipate complications related to obesity and metabolic dysfunction, such as type 2 diabetes and hypertension, rather than the signs of wasting or purging found in restrictive or bulimic disorders.
- Rule in Choice 3: Metabolic syndrome and type 2 diabetes are primary physical risks stemming from the sustained caloric surplus of binging.
- Rule out Choice 1: Lanugo and electrolyte deficits are signs of severe starvation or purging, not binge-eating disorder.
- Rule out Choice 2: Dental erosion is specifically linked to the gastric acid exposure seen in purging behaviors.
- Rule out Choice 4: Cachexia is a state of wasting that is physically incompatible with the diagnostic presentation of binge-eating disorder.
Take home points
- Binge-eating disorder carries significant risks for chronic metabolic diseases, including type 2 diabetes and hypertension.
- Physical complications differ markedly from those of anorexia nervosa or bulimia nervosa.
- Screening for metabolic parameters is a critical component of physical care for clients with this disorder.
- Management requires a dual focus on psychological recovery and the treatment of long-term weight-related health complications.
The nurse is interviewing a client suspected of binge-eating disorder. Which of the following questions would best elicit the core diagnostic feature?
Explanation
Binge-eating disorder is clinically characterized by a profound subjective loss of control over eating during episodes, requiring nurses to ask targeted questions that identify this specific behavioral marker rather than screening for compensatory symptoms.
Rationale for correct answer:
D. Loss of control is the essential, defining feature of a binge episode. Asking about the client’s ability to stop eating helps identify the pathological inability to regulate intake, which confirms the core diagnostic criterion for the disorder.
Rationale for incorrect answers:
A. Self-induced vomiting is a specific compensatory behavior indicative of bulimia nervosa. This question screens for purging methods rather than the binge episodes themselves, making it an ineffective tool for diagnosing binge-eating disorder.
B. Excessive exercise is a compensatory behavior utilized in other eating disorders to mitigate caloric intake. This behavior is not a diagnostic feature of binge-eating disorder and does not assess the primary symptom of uncontrolled overconsumption.
C. Caloric restriction is a primary feature of anorexia nervosa or disordered eating patterns involving starvation. This question screens for restrictive habits that are unrelated to the diagnostic criteria for binge-eating disorder, where intake is characteristically excessive.
Test-taking strategy:
Analyze the scenario/question: The question requires identifying the most effective assessment technique to reveal the core symptom of binge-eating disorder, which is the loss of control during episodes of overconsumption.
Apply knowledge of clinical assessment: Diagnostic assessment must focus on the behaviors defined by the DSM-5. Since the core of binge-eating disorder is the inability to control the binge, the nurse must use an open-ended or direct inquiry that targets the client's subjective experience of that specific event.
- Rule out Choice 1: Purging is an exclusionary feature or a diagnostic sign of a different eating disorder.
- Rule out Choice 2: Excessive exercise is a compensatory behavior not found in the diagnostic criteria for this condition.
- Rule out Choice 3: Caloric restriction is a behavioral hallmark of anorexia, not binge-eating disorder.
- Rule in Choice 4: A sense of loss of control is the fundamental diagnostic element that identifies a true binge episode.
Take home points
- The core diagnostic feature of binge-eating disorder is a subjective loss of control during food consumption episodes.
- Clinical assessment should prioritize identifying the presence of this "loss of control" rather than screening for purging or restrictive behaviors.
- Distinguishing between different eating disorders is critical because their diagnostic criteria and treatment pathways are distinct.
- Use of targeted, patient-centered questions improves the accuracy of psychiatric screening and clinical documentation.
The nurse is selecting a screening approach for binge-eating disorder in a busy outpatient clinic. Which of the following instruments is specifically designed for this purpose?
Explanation
Binge-eating disorder requires the use of specialized screening tools to accurately identify symptomatic behaviors in clinical settings, ensuring that patients receive timely diagnostic evaluation and evidence-based therapeutic interventions.
Rationale for correct answer:
A. The Questionnaire on Eating and Weight Patterns is a validated tool specifically engineered to detect symptoms of binge-eating disorder. It systematically assesses for binge episodes and the associated loss of control, making it ideal for efficient clinical screening.
Rationale for incorrect answers:
B. The Beck Depression Inventory is a widely utilized psychological instrument designed to quantify the severity of depressive symptoms. While depression is a common comorbidity, this tool does not screen for the specific diagnostic features of binge-eating disorder.
C. The Confusion Assessment Method is an instrument utilized for the rapid identification of acute delirium in clinical patients. It is entirely unrelated to the assessment of eating behaviors and the diagnosis of psychiatric feeding conditions.
D. The Abnormal Involuntary Movement Scale is a specialized assessment tool used to screen for tardive dyskinesia in patients receiving antipsychotic medications. It is not an instrument used to identify or characterize disordered eating patterns.
Test-taking strategy:
Analyze the scenario/question: The question asks for the most appropriate clinical instrument to screen for binge-eating disorder in a busy setting, requiring the ability to distinguish between diagnostic tools for eating disorders and those for other psychiatric or physical conditions.
Apply knowledge of screening tools: Selecting the correct tool requires matching the instrument's intended purpose with the clinical objective. Understanding that specific validated questionnaires exist for binge-eating disorder ensures that the nurse provides focused and accurate screening rather than using generic mood or medical assessments.
- Rule in Choice 1: This questionnaire is a validated screening instrument specifically for binge-eating behaviors.
- Rule out Choice 2: The Beck Depression Inventory is focused on mood assessment rather than eating disorder pathology.
- Rule out Choice 3: The Confusion Assessment Method is intended for the diagnosis of acute delirium or altered mental status.
- Rule out Choice 4: The Abnormal Involuntary Movement Scale is dedicated to detecting neurological side effects of medications.
Take home points
- Utilization of validated screening tools is essential for early identification of binge-eating disorder in outpatient clinics.
- The Questionnaire on Eating and Weight Patterns is specifically designed to target binge-eating symptomatology.
- Clinicians must ensure that the screening instrument used aligns with the disorder being investigated to ensure clinical accuracy.
- General psychiatric tools, such as depression inventories, do not adequately capture the diagnostic criteria for eating disorders.
The nurse is performing a physical examination on a client with binge-eating disorder. Which of the following findings would most suggest coexisting insulin resistance?
Explanation
Binge-eating disorder is frequently associated with metabolic derangements including insulin resistance, necessitating that nurses perform targeted physical assessments to identify cutaneous markers that signal underlying endocrine dysfunction.
Rationale for correct answer:
A. Acanthosis nigricans manifests as hyperpigmented, velvety plaques in skin folds, serving as a clinical hallmark of hyperinsulinemia and insulin resistance. This finding reflects the physiological strain placed on the endocrine system due to long-standing caloric surplus and systemic metabolic stress.
Rationale for incorrect answers:
B. Parotid gland swelling (sialadenosis) is a characteristic physical manifestation of chronic self-induced vomiting. This finding is highly specific to bulimia nervosa and is typically absent in patients who do not engage in purging behaviors.
C. Russell's sign consists of calluses or abrasions on the knuckles caused by repeated contact with teeth during induced vomiting. Like parotid enlargement, this physical finding is a diagnostic indicator of purging pathology rather than binge-eating disorder.
D. Lanugo is fine, downy hair that develops as a compensatory response to severe protein-energy malnutrition and starvation states. This clinical sign is observed in anorexia nervosa and is physiologically inconsistent with the excessive intake seen in binge-eating disorder.
Test-taking strategy:
Analyze the scenario/question: The question asks for physical examination findings suggestive of insulin resistance in a client with binge-eating disorder, requiring the differentiation of metabolic markers from physical signs of purging or starvation.
Apply knowledge of physical assessment: Physical examination of clients with eating disorders requires a nuanced understanding of how specific behaviors (purging, starving, or bingeing) manifest physically. Insulin resistance is a common complication of obesity and binge-eating, and nurses must recognize the specific skin changes associated with hyperinsulinemia, such as acanthosis nigricans, to facilitate early metabolic screening.
- Rule in Choice 1: Acanthosis nigricans is a pathognomonic skin marker for hyperinsulinemia and associated insulin resistance.
- Rule out Choice 2: Parotid gland enlargement is a diagnostic marker for purging, not binge-eating.
- Rule out Choice 3: Russell's sign is a specific sign of mechanical injury from purging behaviors.
- Rule out Choice 4: Lanugo is a physical response to severe nutritional deprivation and wasting.
Take home points
- Acanthosis nigricans is a clinical indicator of insulin resistance and should be screened for in clients with binge-eating disorder.
- Physical markers of eating disorders are highly specific to the underlying behavior, whether it be starvation, purging, or bingeing.
- Parotid swelling and Russell's sign are indicative of purging behaviors found in bulimia nervosa.
- Lanugo is associated with the starvation states of anorexia nervosa and is not seen in clients with binge-eating disorder.
The nurse is prioritizing care for several clients with binge-eating disorder. Which of the following clients should the nurse assess first?
Explanation
Binge-eating disorder necessitates nursing prioritization focusing on client safety when assessing for acute psychiatric distress or high-risk behaviors that indicate an immediate threat to the individual's life.
Rationale for correct answer:
C. Hopelessness and thoughts of death represent severe psychiatric symptoms requiring immediate nursing assessment to prevent self-harm. Prioritizing this client is essential to manage the high-risk status associated with major depression in binge-eating disorder.
Rationale for incorrect answers:
A. Embarrassment about eating habits is a common emotional symptom of the disorder. While this finding is clinically relevant for long-term psychological intervention, it does not represent an acute physiological threat or immediate safety risk.
B. Weight gain is a frequently observed physical complication of binge-eating disorder. Although the client requires ongoing monitoring and metabolic screening, this finding is generally stable and does not necessitate immediate nursing prioritization over psychiatric crises.
D. Meal planning discussions indicate the client’s readiness for change and engagement in the therapeutic process. This is a positive development for long-term recovery but is not an urgent clinical concern compared to active suicidal ideation.
Test-taking strategy:
Analyze the scenario/question: The question requires prioritizing nursing assessment for clients with binge-eating disorder, applying principles of triage to distinguish between stable psychological symptoms and acute psychiatric emergencies.
Apply knowledge of safety prioritization: Nursing care prioritization must utilize the hierarchy of clinical urgency. Acute safety risks, particularly suicidal ideation or thoughts of death, take precedence over chronic behavioral patterns, physical health complications, or routine therapeutic planning activities to prevent harm.
- Rule in Choice 3: Suicidal ideation represents an immediate safety crisis and must be assessed first.
- Rule out Choice 1: Feelings of embarrassment are expected symptoms that do not threaten client safety.
- Rule out Choice 2: Weight gain is a chronic physical complication that does not require urgent intervention.
- Rule out Choice 4: A desire for dietary planning is a stable goal unrelated to acute safety risks.
Take home points
- Acute psychiatric emergencies, including thoughts of death or self-harm, are always the top priority in nursing assessment.
- Chronic physical symptoms like weight gain are important but stable, allowing for deferred assessment during crises.
- Psychological symptoms like embarrassment or shame are foundational to the disorder but are not acute threats.
- Readiness for therapeutic engagement, such as meal planning, is a long-term goal that does not override immediate safety needs.
The nurse is formulating a plan of care for a client with binge-eating disorder. Which of the following nursing diagnoses most directly addresses the maladaptive use of food to manage emotion?
Explanation
Binge-eating disorder is a psychiatric condition wherein clients utilize food as a maladaptive mechanism to navigate intense emotional distress, reflecting significant deficits in healthy psychological coping strategies.
Rationale for correct answer:
B. Ineffective coping represents the primary nursing diagnosis for clients who rely on binge eating to regulate their emotional states. This diagnosis directly targets the maladaptive behavior used to mitigate underlying psychological pain or stress.
Rationale for incorrect answers:
A. Fluid volume deficits are typically associated with dehydration or hemorrhage. This diagnosis is clinically irrelevant to binge-eating disorder, which does not involve significant fluid loss or the physiological mechanisms leading to circulatory impairment.
C. Gas exchange impairment refers to respiratory conditions like pneumonia or COPD. This diagnosis pertains strictly to pulmonary function and is not associated with the behavioral or metabolic aspects of disordered eating.
D. Infection risk diagnoses are reserved for clients with compromised immune systems or invasive procedures. Binge-eating disorder does not inherently compromise host defenses or increase susceptibility to pathogenic agents under standard clinical conditions.
Test-taking strategy:
Analyze the scenario/question: The question requires selecting the most appropriate nursing diagnosis for a client who uses food to manage emotions, necessitating an understanding of how behavioral and psychological patterns are mapped to standard nursing diagnoses.
Apply the Nursing Process: A nursing diagnosis must be directly supported by the clinical assessment data. Since the core issue described is the "maladaptive use of food to manage emotion," the diagnosis must address the client's ability to handle stress or emotional triggers. Ineffective coping is the specific diagnostic label used when a client demonstrates a pattern of failed attempts to manage life stressors.
- Rule in Choice 2: Ineffective coping directly addresses the emotional dysregulation and maladaptive behaviors described in the question.
- Rule out Choice 1: Fluid volume status is not a clinical concern in the presentation of binge-eating disorder.
- Rule out Choice 3: Gas exchange is a physiological process unrelated to the psychological pathology of the disorder.
- Rule out Choice 4: Risk for infection is not a relevant diagnostic focus for behavioral or psychological disorders of this type.
Take home points
- Nursing diagnoses for binge-eating disorder must focus on behavioral, psychological, and emotional regulation deficits.
- Ineffective coping is the standard diagnostic choice for patterns of using substances or food as an emotional crutch.
- Physiological diagnoses like gas exchange or fluid volume are generally not applicable to the primary presentation of this disorder.
- Accurate nursing diagnosis facilitates the creation of a targeted, recovery-oriented care plan that addresses the patient's actual needs.
The nurse is establishing goals with a client who has binge-eating disorder. Which of the following represents the most appropriate expected outcome?
Explanation
Binge-eating disorder treatment focuses on psychological stabilization and the acquisition of adaptive skills to manage emotional triggers, fostering a sustainable recovery rather than prioritizing rapid weight loss through restrictive practices.
Rationale for correct answer:
C. Adaptive coping strategies are the primary therapeutic objective for individuals recovering from binge-eating disorder. Identifying emotional triggers and replacing maladaptive eating with healthy regulation behaviors is essential for achieving long-term psychological health and behavioral stability.
Rationale for incorrect answers:
A. Rapid restriction is a dangerous practice that exacerbates the cycle of deprivation and bingeing. Encouraging weight loss through extreme caloric limitation is clinically contraindicated as it undermines the goal of establishing a balanced relationship with food.
B. Carbohydrate elimination promotes a rigid and unsustainable approach to nutrition. Restrictive dieting is a behavioral catalyst for binge episodes, and the goal of recovery is to achieve dietary flexibility rather than adopting restrictive rules.
D. Social disclosure and support are often critical components of the healing process. Encouraging the client to maintain secrecy is detrimental, as it reinforces the shame and isolation that often perpetuate the binge-eating cycle.
Test-taking strategy:
Analyze the scenario/question: The question requires identifying the most appropriate therapeutic outcome for a client with binge-eating disorder, focusing on the principles of evidence-based recovery rather than weight-loss goals.
Apply the goal-setting principle: Expected outcomes in nursing care for eating disorders must be realistic, safe, and focused on behavioral/psychological wellness. Because the disorder is rooted in emotional dysregulation, goals that promote healthy coping, awareness of triggers, and nutritional balance are superior to goals focused solely on weight or restrictive dieting.
- Rule out Choice 1: Rapid weight loss via restriction is a maladaptive trigger that increases the risk of binge relapse.
- Rule out Choice 2: Rigid dietary rules like carbohydrate elimination are contraindicated in binge-eating recovery.
- Rule in Choice 3: Developing adaptive strategies to manage triggers is the cornerstone of sustainable behavioral health.
- Rule out Choice 4: Secrecy is a pathological feature of the disorder that should be addressed, not encouraged.
Take home points
- Treatment goals for binge-eating disorder prioritize emotional regulation and skill-building over rapid weight reduction.
- Restrictive dieting and rigid food rules are triggers for binge-eating relapse and should be avoided in care plans.
- Building a supportive network is an important part of recovery; secrecy should be discouraged.
- Successful recovery is measured by the client's ability to manage emotional distress without resorting to compulsive overconsumption.
The nurse is providing care within the treatment milieu for a client with binge-eating disorder. Which of the following nursing actions best supports recovery?
Explanation
Treatment milieu management in the care of binge-eating disorder focuses on fostering a supportive environment that mitigates shame-based behaviors and promotes the development of adaptive interpersonal connections and self-regulation.
Rationale for correct answer:
C. Nonjudgmental interaction is a foundational component of the therapeutic environment. Consistently providing a shame-free atmosphere enables the client to safely address the emotional triggers that underlie their disorder without the paralyzing fear of clinical stigmatization.
Rationale for incorrect answers:
A. Food restriction is a maladaptive clinical intervention that reinforces the cycle of biological deprivation and psychological tension. Restricting access to food does not teach the client to regulate intake but instead triggers the very overcompensatory behaviors that the treatment milieu aims to resolve.
B. Public recording of weight is highly detrimental to the psychological recovery process. This practice emphasizes external validation over internal growth and exacerbates the body-related shame and self-esteem deficits that are central features of the client's clinical presentation.
D. Discouraging expression regarding eating behaviors inhibits the exploration of core psychological issues. Open communication about eating and emotional states is required for the client to gain insight into their maladaptive behaviors and learn to utilize healthy communication in their recovery.
Test-taking strategy:
Analyze the scenario/question: The question asks to identify the most effective nursing action within a treatment milieu to support the recovery of a client with binge-eating disorder, requiring the application of therapeutic communication principles.
Apply the principles of therapeutic environment: A therapeutic milieu must be designed to promote safety, dignity, and personal growth. In the context of binge-eating disorder, the environment must specifically counteract the themes of secrecy, shame, and judgment that are inherent to the disorder's presentation. Actions that promote self-esteem and open communication are therapeutic, while punitive measures or practices that emphasize weight-focused shame are harmful.
- Rule out Choice 1: Restrictive measures exacerbate metabolic and psychological hunger and undermine recovery goals.
- Rule out Choice 2: Weight-focused public monitoring fosters body dissatisfaction and promotes a culture of shame.
- Rule in Choice 3: Maintaining a nonjudgmental, shame-free environment is essential for successful therapeutic engagement.
- Rule out Choice 4: Limiting the expression of feelings about food prevents the client from developing the necessary insight to change behaviors.
Take home points
- The therapeutic milieu must proactively reduce the shame and secrecy that characterize binge-eating disorder.
- Punitive dietary restrictions and weight-focused monitoring are clinically counterproductive and detrimental to psychological healing.
- Nursing interventions should focus on emotional validation, transparent communication, and creating a safe space for behavioral change.
- Recovery is bolstered when the nurse serves as a consistent, nonjudgmental support figure, enabling the client to confront their challenges openly.
The nurse is reinforcing nutritional teaching for a client with binge-eating disorder. Which of the following statements by the client indicates correct understanding?
Explanation
Nutritional stabilization in binge-eating disorder requires the establishment of consistent intake patterns to maintain metabolic homeostasis, preventing the physiological hunger that often serves as a primary trigger for uncontrolled binge episodes.
Rationale for correct answer:
B. Regular meals and snacks maintain stable blood glucose levels and prevent the intense physiological hunger that leads to binge triggers. This approach fosters a healthy relationship with food and prevents the cycle of deprivation and overconsumption.
Rationale for incorrect answers:
A. Skipping meals is a harmful behavior that promotes extreme hunger and metabolic instability. This pattern of caloric restriction is a known behavioral catalyst that significantly increases the probability of future uncontrolled bingeing events.
C. Fasting completely following a binge episode reinforces a punitive cycle of restriction and compensation. This practice is scientifically counterproductive as it maintains the maladaptive cycle of deprivation, directly undermining the client's efforts toward behavioral change.
D. Strict dieting imposes rigid rules that lead to psychological tension and eventual behavioral failure. A restrictive approach to nutrition is inherently unsustainable and acts as a major behavioral stressor that perpetuates the underlying disorder's pathological cycle.
Test-taking strategy:
Analyze the scenario/question: The question requires identifying the client's understanding of sustainable nutritional strategies for binge-eating disorder recovery, necessitating the differentiation between healthy eating habits and restrictive patterns that induce relapse.
Apply knowledge of nutritional recovery: Recovery from binge-eating disorder relies on breaking the cycle of restriction and bingeing. Nutritional stability through regular, balanced intake is the evidence-based approach to minimize physiological hunger and emotional triggers. Any response favoring restriction, fasting, or rigid control indicates a misunderstanding of the disorder’s behavioral cycle.
- Rule out Choice 1: Skipping meals induces physiological stress and increases the risk of bingeing.
- Rule in Choice 2: Consistent eating patterns are behavioral safeguards that prevent the deprivation-binge cycle.
- Rule out Choice 3: Post-binge fasting is a maladaptive compensatory behavior that reinforces the disorder.
- Rule out Choice 4: Strict dieting is a primary trigger for binge-eating disorder and must be avoided.
Take home points
- Nutritional stability is achieved through consistent, regular eating patterns rather than restriction or fasting.
- Physiological hunger is a major, manageable trigger for binge episodes that is best addressed through routine meals and snacks.
- Restrictive dieting is counterproductive and serves as a direct behavioral catalyst for relapse.
- Successful recovery involves replacing rigid dietary rules with a flexible, balanced approach to nutrition.
The nurse is teaching a client about cognitive-behavioral strategies for binge-eating disorder.
Which of the following techniques should the nurse recommend?
Explanation
Cognitive-behavioral interventions in binge-eating disorder prioritize the development of metacognitive awareness and behavioral self-regulation, enabling clients to systematically identify and modify the psychological patterns that precipitate binge episodes.
Rationale for correct answer:
D. Food and mood diaries serve as essential behavioral tools for gathering data on the environmental and emotional triggers of bingeing. This technique facilitates the identification of maladaptive thought patterns and emotional states, allowing the client and clinician to develop targeted, adaptive coping responses to replace compulsive consumption.
Rationale for incorrect answers:
A. Repeated weighing is a maladaptive behavior that exacerbates body-related distress and reinforces an unhealthy focus on weight as a measure of self-worth. This focus on numerical feedback is counterproductive to recovery and tends to trigger the very emotional turbulence that the client is working to stabilize.
B. Avoiding food situations is an unsustainable and fear-based avoidance strategy that prevents the development of healthy exposure and regulation skills. Learning to interact with food in diverse contexts is a critical milestone for achieving long-term normalization of eating behaviors rather than relying on restrictive environmental control.
C. Compensating behaviors such as skipping meals represent a continuation of the cycle of deprivation and overconsumption. These punitive measures directly undermine the objective of establishing a consistent eating pattern, reinforcing the physiological and psychological triggers that perpetuate the disorder's pathological cycle.
Test-taking strategy:
Analyze the scenario/question: The question asks for effective cognitive-behavioral techniques for managing binge-eating disorder, requiring the identification of strategies that promote self-awareness and regulation rather than those that reinforce shame or restriction.
Apply knowledge of cognitive-behavioral principles: Cognitive-behavioral therapy for binge-eating disorder focuses on identifying the link between thoughts, feelings, and eating behaviors. Effective techniques emphasize tracking patterns, challenging negative self-evaluations, and building adaptive skills, while strategies involving avoidance, rigid control, or punishment are strictly avoided as they sustain the disorder.
- Rule out Choice 1: Frequent weighing is a maladaptive focus that fuels body-related shame and anxiety.
- Rule out Choice 2: Radical avoidance of food is an ineffective coping mechanism that prevents the client from developing regulation skills.
- Rule out Choice 3: Compensatory fasting is a punitive behavior that reinforces the binge-deprivation cycle.
- Rule in Choice 4: Diary tracking provides essential insights into emotional triggers and behavioral patterns for therapeutic change.
Take home points
- Cognitive-behavioral strategies focus on increasing self-awareness regarding the relationship between emotional states and food intake.
- Food and mood logging is a primary tool used to identify the specific triggers that necessitate therapeutic intervention.
- Avoidance, restrictive behaviors, and compensatory fasting are counterproductive and should be replaced by adaptive self-regulation.
- Recovery is an active process of learning to navigate real-world situations while maintaining a consistent and balanced approach to eating.
The nurse is administering medication to a client with moderate-to-severe binge-eating disorder. Which of the following medications is specifically approved for this indication?
Explanation
Binge-eating disorder pharmacotherapy requires the use of Food and Drug Administration (FDA)-approved agents that target the neurobiological pathways involved in compulsive consumption and impulse control, specifically within the context of moderate-to-severe diagnostic presentation.
Rationale for correct answer:
A. Lisdexamfetamine is a stimulant medication specifically approved for the treatment of moderate-to-severe binge-eating disorder. It functions by modulating dopamine and norepinephrine activity in the central nervous system, effectively reducing the frequency of binge episodes and helping to improve behavioral regulation in affected clients.
Rationale for incorrect answers:
B. Haloperidol is a potent typical antipsychotic medication used for the treatment of schizophrenia and severe agitation. It possesses no therapeutic efficacy for binge-eating disorder and is associated with significant neurological side effects, including extrapyramidal symptoms and the risk of tardive dyskinesia.
C. Lithium is a mood stabilizer primarily indicated for the management of bipolar disorder. While it has applications in psychiatric care, it is not an approved or effective treatment for binge-eating disorder and requires strict monitoring of serum levels to prevent acute toxicity.
D. Lorazepam is a benzodiazepine used to treat anxiety, insomnia, and acute seizure activity. It is contraindicated for long-term use in binge-eating disorder due to its sedative profile and the high risk of physical dependence and abuse potential in this vulnerable population.
Test-taking strategy:
Analyze the scenario/question: The question requires identifying the specific pharmacologic agent approved for the treatment of moderate-to-severe binge-eating disorder, necessitating differentiation between approved psychiatric medications and those used for unrelated conditions.
Apply knowledge of psychopharmacology: Clinical practice requires precise knowledge of FDA-approved indications for psychiatric medications. By identifying the stimulant nature of lisdexamfetamine, the nurse can recognize its role in modulating impulse control, whereas the other choices are either antipsychotics, mood stabilizers, or benzodiazepines with distinct therapeutic profiles not indicated for binge-eating disorder.
- Rule in Choice 1: Lisdexamfetamine is the only FDA-approved stimulant indicated for binge-eating disorder.
- Rule out Choice 2: Haloperidol is an antipsychotic medication unrelated to the pathology of eating disorders.
- Rule out Choice 3: Lithium is a mood stabilizer restricted to the management of bipolar affective disorder.
- Rule out Choice 4: Lorazepam is a benzodiazepine that poses risks of dependence and offers no binge-reducing benefits.
Take home points
- Lisdexamfetamine is the primary pharmacologic intervention specifically approved for moderate-to-severe binge-eating disorder.
- Pharmacotherapy should always be integrated into a comprehensive treatment plan that includes psychological therapy and nutritional counseling.
- Stimulant medications like lisdexamfetamine carry risks, including cardiovascular effects and the potential for misuse, requiring careful clinical monitoring.
- Other psychiatric agents, such as antipsychotics or benzodiazepines, are not indicated for this disorder and may cause harmful side effects.
The nurse is caring for a male client who is reluctant to disclose symptoms of binge-eating disorder.
Which of the following understandings should guide the nurse's approach?
Explanation
Binge-eating disorder is a psychiatric condition that affects individuals across all gender identities, yet it remains significantly underrecognized in male populations due to societal stigma and the persistent misperception that eating disorders are exclusively female-associated pathological concerns.
Rationale for correct answer:
C. Underrecognition of binge-eating disorder in male clients is a documented clinical challenge, often stemming from the misconception that these disorders do not affect men. A nurse must employ sensitive screening to overcome the shame and reluctance male clients often feel when discussing these symptoms.
Rationale for incorrect answers:
A. Gender-inclusive occurrence is a well-established clinical fact, as binge-eating disorder affects both men and women. The assumption that this disorder does not exist in males is a dangerous clinical bias that prevents men from accessing essential mental health support.
B. Cognitive-behavioral therapy is highly effective for both men and women struggling with binge-eating disorder. Asserting that male clients cannot benefit from this evidence-based intervention is incorrect and ignores the proven efficacy of skill-based approaches across all gender categories.
D. Weight-neutral diagnosis is a cornerstone of current clinical practice, as binge-eating disorder is not dependent on a specific weight trajectory. Males can and do develop the disorder regardless of their current body mass or any history of weight change, making this diagnostic assumption entirely invalid.
Test-taking strategy:
Analyze the scenario/question: The question asks for the correct nursing perspective on managing binge-eating disorder in males, requiring the identification of common misconceptions and the application of equitable, gender-sensitive clinical practices.
Apply knowledge of gender and eating disorders: Effective nursing care requires recognizing that eating disorders, including binge-eating disorder, transcend gender boundaries. Nurses must actively combat internalized biases and societal stigmas that lead to the under-diagnosis of these conditions in male patients by prioritizing inclusive screening and empathic communication.
- Rule out Choice 1: Eating disorders are not gender-specific conditions and can affect anyone.
- Rule out Choice 2: Behavioral therapies are universally applicable and effective treatments for binge-eating disorder.
- Rule in Choice 3: Sensitivity and proactive screening are necessary to overcome the stigma that prevents males from seeking help.
- Rule out Choice 4: Diagnostic criteria for binge-eating disorder are not contingent on weight loss or specific body types.
Take home points
- Binge-eating disorder is a significant health concern for males, despite being under-diagnosed due to societal stigma.
- Nurses must maintain a bias-free and gender-inclusive approach to screening for all eating disorders.
- Cognitive-behavioral therapy is an effective, evidence-based treatment for all clients, regardless of gender.
- Clinical assumptions about weight or gender should never be used as a basis for excluding a potential diagnosis of binge-eating disorder.
Exams on Binge-Eating Disorder
Custom Exams
Login to Create a Quiz
Click here to loginLessons
- Objectives
- Introduction
- Overview And Epidemiology Of Binge-Eating Disorder
- Etiology And Pathophysiology
- Practice Questions 1
- DSM-5-TR Diagnostic Criteria
- Clinical Manifestations And Complications
- Practice Questions 2
- Nursing Assessment
- Practice Questions 3
- Nursing Diagnoses, Planning, And Outcomes
- Practice Questions 4
- Psychotherapeutic And Pharmacologic Treatment
- Evaluation, Prognosis, And Special Considerations
- Practice Questions 5
- Summary
- Comprehensive Questions
Notes Highlighting is available once you sign in. Login Here.
Objectives
Upon completion of this topic, the learner will be able to:
- Define binge-eating disorder (BED) within the DSM-5-TR framework and trace its historical evolution as a distinct feeding and eating disorder.
- Describe the epidemiology, prevalence, risk factors, protective factors, and comorbidities associated with binge-eating disorder.
- Explain the etiology and pathophysiology of binge-eating disorder, integrating neurobiological, genetic, psychological, and sociocultural determinants.
- Apply the DSM-5-TR diagnostic criteria, severity specifiers, remission classifications, and differential diagnostic reasoning to identify binge-eating disorder.
- Identify the behavioral, psychological, and physical manifestations and the medical complications of recurrent binge eating.
- Perform a comprehensive nursing assessment using validated screening tools, physical examination, psychosocial evaluation, and diagnostic studies.
- Formulate priority nursing diagnoses and establish measurable client-centered goals and expected outcomes.
- Implement evidence-based nursing interventions, including the therapeutic relationship, milieu management, nutritional rehabilitation, cognitive-behavioral strategies, and education.
- Discuss the psychotherapeutic modalities, pharmacologic agents, and interdisciplinary levels of care used in management.
- Evaluate client outcomes, prognosis, relapse-prevention strategies, and special ethical, legal, and population-specific considerations.
Introduction
- Binge-eating disorder (BED) is a psychiatric feeding and eating disorder marked by recurrent episodes of consuming objectively large amounts of food within a discrete period. Each episode is accompanied by a subjective loss of control and marked distress, but without the compensatory behaviors that define bulimia nervosa.
- It was formally recognized as an independent diagnosis in the DSM-5 (2013) and retained with clarified thresholds in the DSM-5-TR (2022). It is now the most prevalent eating disorder, exceeding the combined prevalence of anorexia nervosa and bulimia nervosa.
- Although strongly associated with overweight and obesity, binge-eating disorder is a distinct psychiatric diagnosis rather than a synonym for obesity. It carries a substantial burden of medical morbidity, psychiatric comorbidity, and functional impairment.
- The pathogenesis is multifactorial. It arises from dysregulated reward and impulse-control circuitry, genetic vulnerability, maladaptive emotion-regulation and cognitive processes, and sociocultural pressures relating to weight, dieting, and stigma.
- Nursing care centers on early recognition through nonjudgmental screening, therapeutic communication that reduces shame and secrecy, nutritional and behavioral rehabilitation, and management of coexisting conditions.
- Because the disorder is frequently underdiagnosed and concealed owing to guilt and weight stigma, the nurse plays a pivotal role in destigmatizing the condition and supporting recovery.
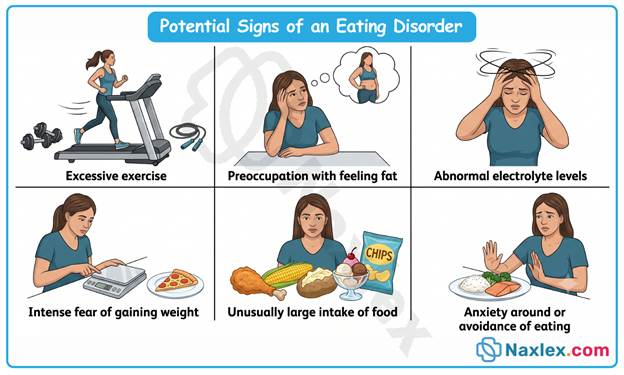
Overview And Epidemiology Of Binge-Eating Disorder
Definition and Historical Context
- Binge-eating disorder is a pattern of recurrent binge-eating episodes. In each episode, the individual consumes, within a discrete period of typically ≤ 2 hours, an amount of food definitively larger than most people would eat in comparable circumstances.
- The episode is defined by a subjective sense of loss of control. The individual feels unable to stop eating or to regulate what or how much is consumed once the episode begins.
- The feature that distinguishes it from bulimia nervosa is the absence of recurrent compensatory behaviors, such as self-induced vomiting, laxative or diuretic misuse, fasting, or excessive exercise.
- The historical evolution of the diagnosis reflects its progressive recognition as a legitimate clinical entity:
- Albert Stunkard first described the phenomenon in 1959, identifying a subgroup of individuals with obesity who exhibited episodic uncontrolled overeating.
- In the DSM-IV (1994), the condition appeared only in Appendix B as a proposed diagnosis for further study. It was captured clinically under the residual category of Eating Disorder Not Otherwise Specified (EDNOS).
- In the DSM-5 (2013), it became a formal, standalone diagnosis. The required threshold was reduced from ≥ 2 binge days per week over 6 months to ≥ 1 binge episode per week over 3 months.
- The DSM-5-TR (2022) retained these criteria without substantive change, while updating the text on prevalence and on culture-related and sex-related features.
- The reduction of the frequency and duration thresholds in the DSM-5 improved diagnostic sensitivity. It reflected evidence that clinically significant impairment occurs even at lower binge frequencies.
Epidemiology and Prevalence
- Binge-eating disorder is the most common eating disorder in the general population. It is especially prevalent among adults presenting for weight-management or bariatric services.
- The lifetime prevalence in adults is estimated at approximately 0.85% to 2.8%. The 12-month prevalence is commonly cited between 0.44% and 1.6%, depending on the population and diagnostic threshold.
- The DSM-5-TR reports a 12-month prevalence of approximately 1.6% among adult females and 0.8% among adult males.
- The sex distribution shows a female-to-male ratio of about 2:1 to 3:1. This is a narrower gender gap than in anorexia nervosa or bulimia nervosa, indicating that the disorder is relatively more common in males than the other primary eating disorders.
- With respect to age of onset, the disorder typically emerges in late adolescence or early adulthood, commonly in the late teens to early 20s. It may begin later than anorexia nervosa or bulimia nervosa and may follow a chronic or remitting-relapsing course.
- Binge-eating disorder occurs across all racial, ethnic, and socioeconomic groups. It is roughly comparably prevalent among diverse populations, contrary to the outdated view that eating disorders mainly affect affluent White females.
- Prevalence is markedly elevated in weight-loss and bariatric surgery populations, where estimates commonly range from approximately 15% to 30% or higher.
- Although strongly correlated with overweight (BMI ≥ 25 kg/m²) and obesity (BMI ≥ 30 kg/m²), the disorder is not synonymous with either and can occur across the full weight spectrum.
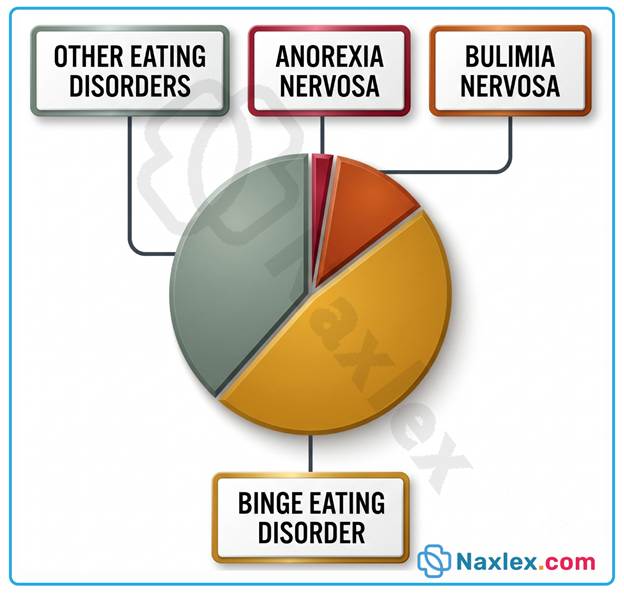
Risk Factors and Protective Factors
- Risk factors are conventionally grouped into predisposing, precipitating, and perpetuating categories that interact across the lifespan.
- Biological and genetic risk factors raise baseline vulnerability:
- A family history of eating disorders, obesity, mood disorders, or substance use disorders elevates risk.
- Heritable temperament traits, including high impulsivity and heightened reward sensitivity, predispose to disordered eating.
- Female sex confers increased risk, though the disparity is smaller than in other eating disorders.
- Psychological risk factors reflect the internal vulnerabilities that drive binge behavior:
- Low self-esteem, negative body image, and pervasive body dissatisfaction are strongly associated.
- Perfectionism, harm avoidance, and difficulty identifying and regulating emotions (alexithymia) contribute significantly.
- A history of depression, anxiety, or other mood disturbance heightens susceptibility.
- Emotional eating, in which food is used to regulate negative affect, perpetuates the pattern.
- Developmental and environmental risk factors shape long-term vulnerability:
- Childhood adversity, including physical, sexual, or emotional abuse and neglect, is a well-established contributor.
- Early exposure to dieting, food restriction, or family preoccupation with weight increases risk.
- Weight-related teasing, bullying, or stigmatization is strongly implicated.
- Food insecurity and irregular eating patterns further predispose to binge eating.
- Precipitating factors that trigger onset include acute psychosocial stressors, interpersonal conflict, loss, major life transitions, and the initiation of restrictive dieting, which can paradoxically provoke binges through deprivation.
- Perpetuating factors that maintain the disorder include the dietary restraint–binge cycle, the reinforcing shame and guilt that follow binges, and the compounding effects of weight stigma and social isolation.
- Protective factors buffer against the disorder:
- Secure attachment and supportive family relationships promote resilience.
- Positive body image, high self-esteem, and effective emotion-regulation skills reduce vulnerability.
- Regular, structured eating patterns and balanced nutrition guard against the restriction-binge cycle.
- Strong social support, media literacy, and resistance to the thin ideal are protective.
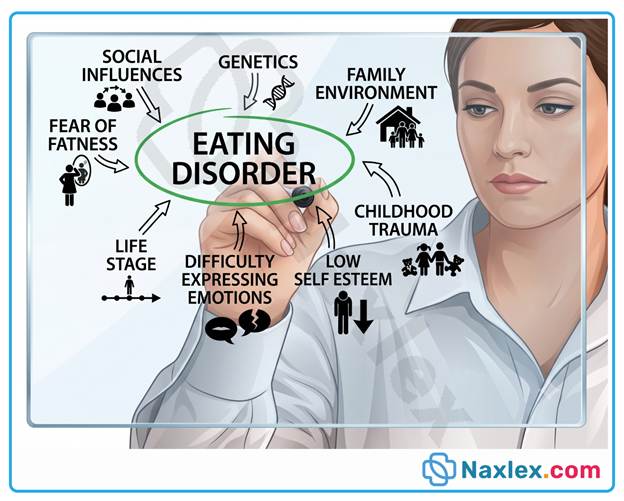
Psychiatric and Medical Comorbidities
- Binge-eating disorder is associated with high rates of comorbidity across psychiatric and medical domains. These conditions increase clinical complexity, complicate treatment, and worsen prognosis.
- Psychiatric comorbidities are common and frequently perpetuate the eating disorder:
- Major depressive disorder and other depressive disorders are the most frequent psychiatric comorbidities.
- Anxiety disorders, including generalized anxiety disorder, social anxiety disorder, and panic disorder, are commonly present.
- Bipolar and related disorders occur at elevated rates.
- Substance use disorders, including alcohol use disorder, share underlying reward and impulsivity pathways.
- Attention-deficit/hyperactivity disorder is linked through shared impulsivity.
- Post-traumatic stress disorder and personality disorders, particularly borderline personality disorder, frequently coexist.
- The risk of suicidal ideation and behavior is elevated relative to the general population.
- Medical comorbidities are largely mediated by obesity and metabolic dysregulation, though independent associations also exist:
- Obesity and its wide-ranging sequelae are the most prominent.
- Type 2 diabetes mellitus, insulin resistance, dyslipidemia, and hypertension are frequently present.
- Metabolic syndrome and cardiovascular disease contribute to long-term morbidity and mortality.
- Gastroesophageal reflux disease and other gastrointestinal disturbances are common.
- Obstructive sleep apnea, chronic pain and musculoskeletal disorders, and menstrual irregularities or polycystic ovary syndrome in females further compound the picture.
Table 3.4.1 Common Comorbidities in Binge-Eating Disorder
|
Category |
Representative Conditions |
Clinical Significance |
|
Mood disorders |
Major depressive disorder, bipolar disorder |
Most frequent psychiatric comorbidity; worsens binge severity and elevates suicide risk |
|
Anxiety disorders |
GAD, social anxiety, panic disorder |
Frequently precede eating disorder onset; drive negative-affect-triggered binges |
|
Substance use disorders |
Alcohol use disorder, other substances |
Share impulsivity and reward-dysregulation pathways |
|
Impulse-control–related |
ADHD |
Shared neurobiology of impulsivity; complicates treatment |
|
Metabolic |
Type 2 diabetes, dyslipidemia, metabolic syndrome |
Contribute to cardiovascular morbidity and mortality |
|
Cardiovascular |
Hypertension, coronary artery disease |
Long-term consequences of obesity and metabolic derangement |
|
Other physical |
OSA, GERD, PCOS, chronic pain |
Reduce quality of life and functional capacity |
- The presence of comorbid conditions necessitates integrated, interdisciplinary assessment and treatment planning. Untreated psychiatric comorbidity frequently perpetuates binge-eating behavior and undermines recovery.
Etiology And Pathophysiology
The etiology of binge-eating disorder is multifactorial and best understood through the biopsychosocial model. No single cause is sufficient. Instead, biological vulnerability interacts with psychological and environmental triggers.
Neurobiological Factors
- Binge-eating disorder involves dysregulation of the brain reward system.
- The mesolimbic dopamine pathway is central to this process.
- Highly palatable foods trigger exaggerated dopamine release.
- Over time, this produces reward hyposensitivity and compulsive overeating.
- Impaired impulse control is linked to prefrontal cortex dysfunction.
- The prefrontal cortex normally inhibits urges and regulates behavior.
- Reduced prefrontal top-down control weakens restraint during cravings.
- Serotonin dysregulation contributes to mood instability and appetite disturbance.
- Low serotonergic tone is associated with impulsivity and negative affect.
- Appetite-regulating hormones are also implicated:
- Leptin signals satiety; leptin resistance blunts fullness cues.
- Ghrelin stimulates hunger and may be dysregulated in binge episodes.
- Insulin resistance frequently coexists and disrupts metabolic signaling.
- Dysfunction of the hypothalamic hunger-satiety centers perpetuates disordered intake.
Genetic and Familial Factors
- Binge-eating disorder demonstrates strong heritability.
- Twin and family studies estimate heritability at approximately 41% to 57%.
- First-degree relatives of affected individuals show elevated risk.
- The disorder aggregates within families alongside obesity and mood disorders.
- Candidate genes involve dopamine and serotonin neurotransmitter systems.
- Polymorphisms affecting reward signaling increase susceptibility.
- Shared familial environment also transmits risk.
- Modeling of disordered eating and dieting behavior is learned within families.
- Familial preoccupation with weight and shape reinforces vulnerability.
Psychological Factors
- Impaired emotion regulation is a core psychological mechanism.
- Binge eating functions as a maladaptive strategy to escape negative affect.
- Negative affect (sadness, anxiety, boredom, anger) frequently precedes binges.
- Eating temporarily reduces distress, reinforcing the behavior.
- The cycle produces subsequent guilt, shame, and self-criticism.
- Cognitive distortions maintain the disorder.
- Distortions include all-or-nothing thinking about food and rigid dietary rules.
- Violation of rules triggers disinhibited overeating (the "what-the-hell" effect).
- Low self-esteem and body dissatisfaction are strongly associated.
- A history of childhood trauma and adversity increases risk.
- Alexithymia (difficulty identifying emotions) impairs adaptive coping.
Sociocultural and Environmental Factors
- The thin ideal promoted by media contributes to body dissatisfaction.
- Internalization of unrealistic body standards drives dieting behavior.
- Weight stigma and weight-based teasing are potent risk factors.
- Stigmatization increases shame, isolation, and further binge eating.
- Chronic dieting and restriction paradoxically precipitate binges.
- Restriction produces physiological and psychological deprivation.
- The obesogenic environment increases access to palatable, energy-dense foods.
- Food insecurity is associated with binge eating and irregular intake.
- Stressful life events and interpersonal conflict act as acute triggers.
DSM-5-TR Diagnostic Criteria
Core Diagnostic Criteria
- The DSM-5-TR classifies binge-eating disorder within Feeding and Eating Disorders.
- Diagnosis requires recurrent episodes of binge eating.
- A binge episode is defined by both of the following:
- Eating, within a discrete period (e.g., ≤ 2 hours), an amount of food definitely larger than most people would eat in similar circumstances.
- A sense of loss of control over eating during the episode.
- Binge episodes are associated with ≥ 3 of the following features:
- Eating much more rapidly than normal.
- Eating until feeling uncomfortably full.
- Eating large amounts when not physically hungry.
- Eating alone due to embarrassment about quantity.
- Feeling disgusted, depressed, or very guilty afterward.
- Marked distress regarding binge eating is present.
- Binge eating occurs, on average, ≥ 1 day per week for ≥ 3 months.
- Binge eating is NOT associated with recurrent inappropriate compensatory behaviors.
- It does not occur exclusively during anorexia nervosa or bulimia nervosa.
Severity Specifiers and Remission Status
- Severity is graded by the frequency of binge-eating episodes per week.
- Severity may be increased to reflect degree of disability.
Table 6.2.1 DSM-5-TR Severity Specifiers for Binge-Eating Disorder
|
Severity |
Binge-Eating Episodes per Week |
|
Mild |
1 to 3 episodes |
|
Moderate |
4 to 7 episodes |
|
Severe |
8 to 13 episodes |
|
Extreme |
≥ 14 episodes |
- Remission status is also specified:
- In partial remission: after full criteria were met, binge eating occurs at an average frequency of < 1 episode per week for a sustained period.
- In full remission: after full criteria were met, none of the criteria have been met for a sustained period.
Differential Diagnosis
- Accurate diagnosis requires excluding overlapping conditions.
- Bulimia nervosa is the key differential.
- Bulimia nervosa includes recurrent inappropriate compensatory behaviors.
- Binge-eating disorder lacks these compensatory behaviors.
- Obesity without binge eating must be distinguished.
- Obesity is not a mental disorder and lacks loss of control.
- Binge-eating disorder is defined by psychological distress and loss of control.
- Mood disorders may involve increased appetite.
- Overeating in depression usually lacks the discrete loss-of-control binge.
- Other conditions to differentiate:
- Bulimia nervosa (compensatory behaviors present).
- Anorexia nervosa, binge-eating/purging type (occurs with low weight and restriction).
- Kleine-Levin syndrome and certain neurologic conditions.
- Medication-induced increased appetite.
Table 6.3.1 Differentiating Binge-Eating Disorder from Bulimia Nervosa
|
Feature |
Binge-Eating Disorder |
Bulimia Nervosa |
|
Binge episodes |
Present |
Present |
|
Loss of control |
Present |
Present |
|
Compensatory behaviors |
Absent |
Present (purging, fasting, exercise) |
|
Typical weight |
Often overweight/obese |
Often normal weight |
|
Self-evaluation |
Distress over binges |
Unduly influenced by shape/weight |
Nursing Insights
- Loss of control, not the amount of food alone, is the defining feature the nurse must identify during assessment.
- The absence of compensatory behaviors is what distinguishes binge-eating disorder from bulimia nervosa, a frequently tested NCLEX point.
- A frequency of ≥ 1 binge per week for ≥ 3 months is required for diagnosis; the nurse should quantify episodes precisely when gathering the history.
Clinical Manifestations And Complications
The clinical presentation of binge-eating disorder encompasses behavioral, psychological, and physical domains. Manifestations are frequently concealed by the client owing to shame and secrecy, which contributes to underrecognition. The nurse must therefore recognize both the overt and the subtle indicators of the disorder.
Behavioral and Psychological Manifestations
- The hallmark behavioral feature is the recurrent binge episode, during which the client consumes an objectively large quantity of food while experiencing a subjective loss of control.
- Clients frequently engage in secretive eating, consuming food alone or hiding evidence such as wrappers and containers because of profound embarrassment about the quantity eaten.
- Eating typically occurs much more rapidly than normal, and the client often continues until becoming uncomfortably or even painfully full.
- Clients commonly eat large amounts of food when not physically hungry, indicating that the eating is driven by emotional rather than physiological cues.
- Hoarding or stockpiling of food, along with disappearance of large amounts of food from the household, may be reported by family members.
- Chaotic and irregular eating patterns are common, frequently alternating between periods of restrictive dieting and episodes of disinhibited overeating.
- Psychologically, the client experiences marked distress, including intense guilt, shame, disgust, and depressed mood following binge episodes.
- Body dissatisfaction, low self-esteem, and preoccupation with weight, shape, and food are pervasive and reinforce the disordered cycle.
- Negative affective states such as anxiety, sadness, boredom, and loneliness frequently precede and trigger binge episodes, while the eating temporarily relieves the distress.
- Social withdrawal and avoidance of situations involving food, such as shared meals, may develop as the client attempts to conceal the behavior.
- Fluctuations in mood and heightened impulsivity are commonly observed and may reflect coexisting psychiatric comorbidity.
Physical Manifestations and Medical Complications
- The physical consequences of binge-eating disorder are largely mediated by weight gain, obesity, and the resulting metabolic derangements, though psychological distress contributes independently to morbidity.
- Many clients present with overweight or obesity, reflected in an elevated body mass index (BMI ≥ 25 kg/m² or ≥ 30 kg/m² respectively), although the disorder can occur across the entire weight spectrum.
- Weight cycling, characterized by repeated loss and regain of body weight, is common and carries its own metabolic and cardiovascular risks.
- Metabolic complications frequently develop and include type 2 diabetes mellitus, insulin resistance, dyslipidemia, and the constellation known as metabolic syndrome.
- Cardiovascular complications include hypertension, coronary artery disease, and an elevated long-term risk of cardiovascular events.
- Gastrointestinal disturbances are prominent and include gastroesophageal reflux disease, abdominal distension, bloating, delayed gastric emptying, and, rarely, acute gastric dilatation from massive overconsumption.
- Musculoskeletal complications such as chronic joint pain, osteoarthritis, and reduced mobility arise from the mechanical burden of excess body weight.
- Obstructive sleep apnea, dyspnea, and reduced exercise tolerance are frequently associated with obesity in these clients.
- Endocrine and reproductive disturbances, including menstrual irregularities and polycystic ovary syndrome, may occur in affected females.
- General fatigue, reduced functional capacity, and diminished quality of life accompany the chronic physical burden of the disorder.
Table 7.2.1 Systemic Complications of Binge-Eating Disorder
|
Body System |
Common Complications |
|
Metabolic/Endocrine |
Type 2 diabetes, insulin resistance, dyslipidemia, metabolic syndrome, PCOS |
|
Cardiovascular |
Hypertension, coronary artery disease, elevated cardiac risk |
|
Gastrointestinal |
GERD, bloating, delayed gastric emptying, rare gastric dilatation |
|
Respiratory |
Obstructive sleep apnea, dyspnea, reduced exercise tolerance |
|
Musculoskeletal |
Osteoarthritis, chronic joint pain, impaired mobility |
|
Reproductive |
Menstrual irregularities, subfertility |
Nursing Assessment
A comprehensive nursing assessment of the client with binge-eating disorder integrates history taking, physical examination, and psychosocial evaluation. Because clients frequently conceal their symptoms, the nurse must establish trust and employ a nonjudgmental, empathetic approach. Accurate assessment forms the foundation for diagnosis, treatment planning, and monitoring of complications.
History Taking and Screening Tools
- The nurse should obtain a detailed eating history, including the frequency, duration, timing, and circumstances of binge episodes, as well as the presence or absence of compensatory behaviors.
- It is essential to elicit the client's subjective experience of loss of control, since this feature is central to the diagnosis and cannot be inferred from food quantity alone.
- A thorough weight history should be gathered, documenting patterns of weight gain, weight cycling, dieting attempts, and the client's perceptions of body weight and shape.
- The nurse should assess for emotional triggers, exploring the relationship between negative affect, stress, and the onset of binge episodes.
- A complete psychiatric history is necessary to identify comorbid mood disorders, anxiety disorders, substance use disorders, and suicidal ideation.
- Validated screening tools enhance detection and structured assessment, including:
- The Binge Eating Scale (BES), which measures the severity of binge-eating behaviors and associated cognitions.
- The Eating Disorder Examination Questionnaire (EDE-Q), a self-report measure of eating-disorder psychopathology.
- The Questionnaire on Eating and Weight Patterns (QEWP), designed specifically to screen for binge-eating disorder.
- The SCOFF questionnaire, a brief general eating-disorder screening instrument.
- The nurse must approach questioning with sensitivity, recognizing that shame and stigma may lead the client to minimize or deny symptoms.
Physical Assessment
- The physical examination begins with accurate measurement of height, weight, and calculation of the body mass index to classify weight status and monitor trends over time.
- Vital signs, including blood pressure and heart rate, should be assessed to detect hypertension and cardiovascular strain associated with obesity.
- The nurse should examine for physical signs of metabolic and cardiovascular complications, such as acanthosis nigricans, which suggests insulin resistance.
- Assessment of the cardiovascular and respiratory systems is important to identify signs of hypertension, heart disease, and obstructive sleep apnea.
- The abdominal examination may reveal distension, tenderness, or discomfort related to overconsumption and gastrointestinal complications.
- The nurse should evaluate the client's mobility, joint function, and skin integrity, particularly in clients with significant obesity.
- General inspection may reveal fatigue, reduced exercise tolerance, and other indicators of the physical burden of the disorder.
Psychosocial and Mental Status Assessment
- The nurse conducts a thorough mental status examination, evaluating mood, affect, thought content, insight, and judgment.
- Assessment of mood and affect is critical, given the strong association between binge-eating disorder and depressive and anxiety disorders.
- The nurse must directly and sensitively assess for suicidal ideation, intent, and plan, as suicide risk is elevated in this population.
- Evaluation of self-esteem, body image, and the degree to which self-worth is influenced by weight and shape provides insight into the client's psychopathology.
- The nurse should explore the client's coping mechanisms, emotion-regulation abilities, and the function that binge eating serves in managing distress.
- Assessment of the client's social support system, interpersonal relationships, and occupational or academic functioning helps identify stressors and resources.
- Exploration of any history of trauma, abuse, or weight-based stigmatization is important, as these are significant contributing factors.
Diagnostic and Laboratory Studies
- Although binge-eating disorder is diagnosed clinically, laboratory and diagnostic studies are essential to detect and monitor associated medical complications.
- A fasting blood glucose and glycated hemoglobin (HbA1c) are obtained to screen for insulin resistance and type 2 diabetes mellitus.
- A lipid panel is indicated to detect dyslipidemia and assess cardiovascular risk.
- Liver function tests may be performed to evaluate for hepatic steatosis (fatty liver disease) associated with obesity.
- A complete metabolic panel, including electrolytes and renal function, provides baseline data and detects metabolic disturbances.
- Thyroid function tests help exclude endocrine contributors to weight change.
- Additional studies, such as an electrocardiogram, sleep study, or evaluation for polycystic ovary syndrome, may be indicated based on clinical findings.
- The nurse should ensure that baseline data are obtained before initiating pharmacologic therapy, particularly when agents affecting cardiac or metabolic parameters are considered.
Table 9.4.1 Common Diagnostic Studies in Binge-Eating Disorder
|
Study |
Purpose |
|
Fasting glucose, HbA1c |
Screen for insulin resistance and type 2 diabetes |
|
Lipid panel |
Detect dyslipidemia, assess cardiovascular risk |
|
Liver function tests |
Evaluate for hepatic steatosis |
|
Complete metabolic panel |
Assess electrolytes, renal function, baseline data |
|
Thyroid function tests |
Exclude endocrine causes of weight change |
|
ECG, sleep study, PCOS workup |
Evaluate cardiac, respiratory, reproductive complications |
Nursing Diagnoses, Planning, And Outcomes
Nursing interventions for binge-eating disorder are evidence-based, collaborative, and directed toward interrupting the binge cycle while addressing the underlying psychological and nutritional disturbances. The nurse implements care within an interdisciplinary framework. Interventions are individualized according to the client's specific needs and comorbidities.
Therapeutic Nurse-Client Relationship and Milieu Management
- The foundation of effective nursing care is the establishment of a therapeutic relationship built on trust, empathy, and unconditional positive regard.
- The nurse must adopt a nonjudgmental stance, recognizing that shame and stigma are central to the client's experience and that criticism will reinforce secrecy.
- The nurse should encourage the client to verbalize feelings, using therapeutic communication techniques such as active listening, reflection, and open-ended questioning.
- Within the treatment milieu, the nurse promotes a structured, supportive environment that provides consistency, predictability, and appropriate limit-setting.
- The nurse observes eating patterns during meals in inpatient or residential settings, providing support and gentle guidance without conveying surveillance or judgment.
- The nurse reinforces the client's autonomy and active participation in the plan of care to enhance self-efficacy and engagement.
- Consistent, respectful, and shame-free interactions across the team are essential to counter the weight stigma that clients frequently encounter.
Nutritional Interventions
- Nutritional interventions are delivered in collaboration with a registered dietitian and aim to normalize eating rather than to impose restriction.
- The nurse supports the establishment of a structured eating pattern consisting of regular meals and planned snacks to prevent the deprivation that precipitates binges.
- The nurse educates the client that rigid dieting and restriction are counterproductive, as they perpetuate the restriction-binge cycle.
- Mechanical eating, in which the client eats at planned times regardless of hunger or emotional state, may be used initially to interrupt chaotic patterns.
- The nurse assists the client in distinguishing physiological hunger from emotional hunger and in reconnecting with internal satiety cues.
- Principles of balanced, adequate nutrition are reinforced, promoting a sustainable and non-punitive approach to food.
- The nurse monitors and documents dietary intake, weight trends, and the client's response to nutritional interventions.
Behavioral and Cognitive Interventions
- Behavioral and cognitive interventions target the maladaptive thoughts and behaviors that maintain the disorder and are grounded in cognitive-behavioral principles.
- The nurse encourages self-monitoring through the use of a food and mood diary, which helps the client identify patterns, triggers, and antecedents of binge episodes.
- The nurse assists the client in recognizing and challenging cognitive distortions, such as all-or-nothing thinking and rigid dietary rules.
- Stimulus-control strategies are taught, such as avoiding cues that trigger binges and restructuring the eating environment.
- The nurse helps the client develop alternative, adaptive coping strategies for managing negative affect, including relaxation techniques, physical activity, and social connection.
- Problem-solving skills and delay techniques (e.g., postponing a binge urge and engaging in a substitute activity) are reinforced.
- The nurse supports the practice of skills learned in formal psychotherapy and reinforces positive behavioral change with encouragement.
Client and Family Education
- Client and family education is a cornerstone of nursing management and promotes understanding, adherence, and sustained recovery.
- The nurse educates the client and family about the nature of binge-eating disorder as a legitimate psychiatric condition rather than a failure of willpower.
- Education addresses the restriction-binge cycle, the role of emotional triggers, and the rationale for structured eating and psychotherapy.
- The nurse provides instruction on prescribed medications, including their purpose, expected effects, and potential adverse effects.
- The family is educated on how to provide supportive, nonjudgmental encouragement and to avoid comments about weight, shape, or eating that reinforce shame.
- The nurse informs the client and family about available community resources, support groups, and follow-up services.
- Education emphasizes the importance of adherence to the treatment plan and early recognition of warning signs of relapse.
Nursing Insights
- The primary treatment goal is reduction of binge episodes and normalization of eating, not weight loss; framing care around weight reinforces shame and undermines recovery.
- A nonjudgmental, shame-free therapeutic relationship is the single most important nursing intervention, because secrecy and stigma are central barriers to disclosure and treatment.
- The nurse must teach that restrictive dieting perpetuates rather than resolves binge eating, as deprivation triggers the very episodes the client is trying to prevent.
Psychotherapeutic And Pharmacologic Treatment
The treatment of binge-eating disorder is multimodal, combining psychotherapy, pharmacologic agents, and interdisciplinary coordination. Psychotherapy is the first-line and most effective intervention, while pharmacotherapy serves an adjunctive role. Treatment is individualized according to symptom severity, comorbidity, and client preference.
Psychotherapy Modalities
- Cognitive-behavioral therapy (CBT) is the first-line and most strongly evidence-supported treatment for binge-eating disorder.
- CBT targets the maladaptive thoughts, dietary rules, and behaviors that maintain the binge cycle, and it produces significant reductions in binge frequency.
- Interpersonal psychotherapy (IPT) is an effective alternative that addresses the interpersonal difficulties and relational contexts underlying binge eating.
- Dialectical behavior therapy (DBT) focuses on emotion regulation and distress tolerance and is particularly useful when affect dysregulation drives binge episodes.
- Guided self-help based on cognitive-behavioral principles is an effective, lower-intensity option for appropriate clients.
- Behavioral weight-loss programs may address weight and metabolic complications but are less effective than CBT for reducing core binge-eating behavior.
- The nurse reinforces the skills and insights developed in formal therapy and supports the client's consistent engagement across sessions.
Pharmacologic Therapy
- Pharmacotherapy is generally adjunctive to psychotherapy and is used to reduce binge frequency and to address comorbid conditions.
- Lisdexamfetamine dimesylate (Vyvanse) is the only agent specifically approved by the U.S. FDA for the treatment of moderate-to-severe binge-eating disorder in adults.
- It is a central nervous system stimulant that reduces binge frequency, and it carries risks including increased heart rate, elevated blood pressure, insomnia, decreased appetite, and potential for misuse.
- The nurse must monitor cardiovascular parameters and assess for a history of substance misuse before and during therapy.
- Selective serotonin reuptake inhibitors (SSRIs), such as fluoxetine and sertraline, are commonly used off-label and are especially beneficial when comorbid depression or anxiety is present.
- Topiramate, an anticonvulsant, reduces binge frequency and promotes weight loss but is limited by adverse effects such as cognitive slowing, paresthesia, and sedation.
- The nurse provides education on the purpose, expected effects, adverse effects, and importance of adherence for all prescribed medications.
- Baseline and ongoing monitoring of vital signs, weight, and relevant laboratory parameters is essential during pharmacologic therapy.
Nursing Insights
- Lisdexamfetamine (Vyvanse) is the only FDA-approved medication for binge-eating disorder; the nurse must monitor blood pressure and heart rate and screen for substance misuse potential, a high-yield NCLEX point.
- Cognitive-behavioral therapy is first-line; medication is adjunctive, and the nurse should reinforce that psychotherapy, not pharmacotherapy, is the cornerstone of treatment.
- Because SSRIs treat coexisting depression and anxiety, the nurse must continue to monitor for suicidal ideation, particularly early in therapy and in clients with comorbid mood disorders.
Interdisciplinary Collaboration and Levels of Care
- Effective management requires a coordinated interdisciplinary team, including the psychiatric provider, primary care provider, registered dietitian, psychotherapist, and nurse.
- The nurse frequently serves as the coordinator and advocate, ensuring continuity of care and communication among team members.
- The appropriate level of care is determined by symptom severity, medical stability, psychiatric acuity, and the client's support system.
- Outpatient care is appropriate for medically stable clients with adequate support and lower symptom severity.
- Intensive outpatient and partial hospitalization programs provide more structured support for clients requiring greater intervention.
- Inpatient or residential care is reserved for clients with severe symptoms, significant medical or psychiatric instability, or high suicide risk.
- The nurse participates in ongoing reassessment to ensure the client is treated at the least restrictive, most appropriate level of care.
Evaluation, Prognosis, And Special Considerations
Evaluation of the client with binge-eating disorder is an ongoing and dynamic process that measures progress against established outcomes. Prognosis is influenced by early intervention, treatment adherence, and management of comorbidities. Special populations and ethical considerations require individualized, sensitive care.
Evaluation of Client Outcomes
- Evaluation is based on the degree to which the client has achieved the measurable goals established in the plan of care.
- The nurse assesses for a reduction in the frequency and severity of binge episodes as a primary indicator of treatment response.
- The client's use of adaptive coping strategies in place of binge eating is evaluated as evidence of psychological progress.
- Improvement in mood, self-esteem, and body image is assessed, along with stabilization of comorbid psychiatric symptoms.
- Stabilization or improvement of metabolic and cardiovascular parameters is monitored as an indicator of physical health.
- The nurse documents findings objectively and revises the plan of care when goals are not being met.
Prognosis and Relapse Prevention
- The prognosis of binge-eating disorder is generally favorable when treatment is timely and comprehensive, though the disorder may follow a chronic or relapsing course.
- Early intervention, treatment adherence, and management of comorbidities are associated with more favorable outcomes.
- Relapse prevention is an essential component of long-term care and requires ongoing support and skill maintenance.
- The nurse assists the client in identifying early warning signs of relapse, such as the return of restrictive dieting or negative-affect-driven eating.
- The client is supported in developing and rehearsing a relapse-prevention plan that includes coping strategies and access to support resources.
- Continued engagement with follow-up care and support groups reinforces sustained recovery.
Special Populations and Legal-Ethical Considerations
- Care must be adapted for special populations, including children and adolescents, older adults, males, and clients from diverse cultural backgrounds.
- Binge-eating disorder in males is frequently underrecognized owing to the misperception that eating disorders affect only females, requiring heightened clinical vigilance.
- Cultural sensitivity is essential, as the expression, perception, and disclosure of symptoms vary across cultural contexts.
- Ethical principles of autonomy, beneficence, nonmaleficence, and confidentiality must guide all aspects of care.
- The nurse advocates for the client, respects the client's right to participate in decisions, and works to reduce weight stigma within the healthcare setting.
- Legal considerations, including informed consent and, in rare cases involving imminent risk, involuntary treatment, must be managed in accordance with professional and jurisdictional standards.
Summary
- Binge-eating disorder is the most prevalent eating disorder and is characterized by recurrent binge episodes with a subjective loss of control and marked distress, in the absence of compensatory behaviors.
- It was formally recognized as a distinct diagnosis in the DSM-5 (2013) and retained in the DSM-5-TR (2022), requiring binge eating on average ≥ 1 day per week for ≥ 3 months.
- The etiology is multifactorial, integrating neurobiological reward and impulse-control dysregulation, genetic and familial heritability, psychological factors such as impaired emotion regulation, and sociocultural influences including the thin ideal and weight stigma.
- Clinical manifestations span behavioral, psychological, and physical domains, with medical complications largely mediated by obesity, including type 2 diabetes, dyslipidemia, hypertension, and cardiovascular disease.
- Comprehensive nursing assessment employs sensitive history taking, validated screening tools, physical examination, mental status evaluation, and laboratory studies to detect complications.
- Priority nursing diagnoses address nutrition, coping, body image, self-esteem, and suicide risk, with goals centered on reducing binge behavior and normalizing eating rather than on weight loss.
- Nursing interventions emphasize a nonjudgmental therapeutic relationship, structured nutritional rehabilitation, cognitive-behavioral strategies, and client and family education.
- Cognitive-behavioral therapy is the first-line treatment, lisdexamfetamine is the only FDA-approved medication, and SSRIs and topiramate serve adjunctive roles within an interdisciplinary model of care.
- Evaluation is ongoing, prognosis is favorable with early comprehensive treatment, and relapse prevention, care of special populations, and adherence to ethical-legal principles are integral to nursing management.
Naxlex
Videos
Login to View Video
Click here to loginTake Notes on Binge-Eating Disorder
This filled cannot be empty
Join Naxlex Nursing for nursing questions & guides! Sign Up Now
